Last week, we discussed change in transmitral filling patterns as the severity of diastolic dysfunction progresses. When we evaluate for diastolic dysfunction, our goal is to determine:
We are able to determine if the LV filling pressures are elevated or not by determining the left atrial pressure (LAP). There are various terms that describe elevated LV filling pressures: elevated LAP or elevated LVEDP. It is common for these terms to be used in conjunction with each other but all referring to the same concept: ventricle being unable to fill properly at a low pressure state, causing an increase in end-diastolic pressures in response to a stiff, non-compliant ventricle.
Echocardiography is unable to directly measure LV filling pressures. Instead, we use a combination of indexes. Since LAP correlates to the invasively-obtained LVEDP, we can evaluate a series of measurements to help us determine if the LAP is elevated or not.
NOTE: The goal of this blog is to have a basic understanding of how these individual indexes play physiological role in elevated LAP. The ASE provides two algorithms to use in conjunction with other indexes to determine both grade of diastolic dysfunction and presence of elevated LAP. Please refer back to our guest speaker blogs to view this information.
The pulmonary artery pressure (PAP) is the most valuable parameter that provides a direct estimate of the LVEDP (in absence of pulmonary arterial disease). An elevated PAP is strongly suggestive of an elevated LAP. The presence of mitral regurgitation, which can elevate the PAP, must be taken into consideration when using this method as an indicator of LAP.
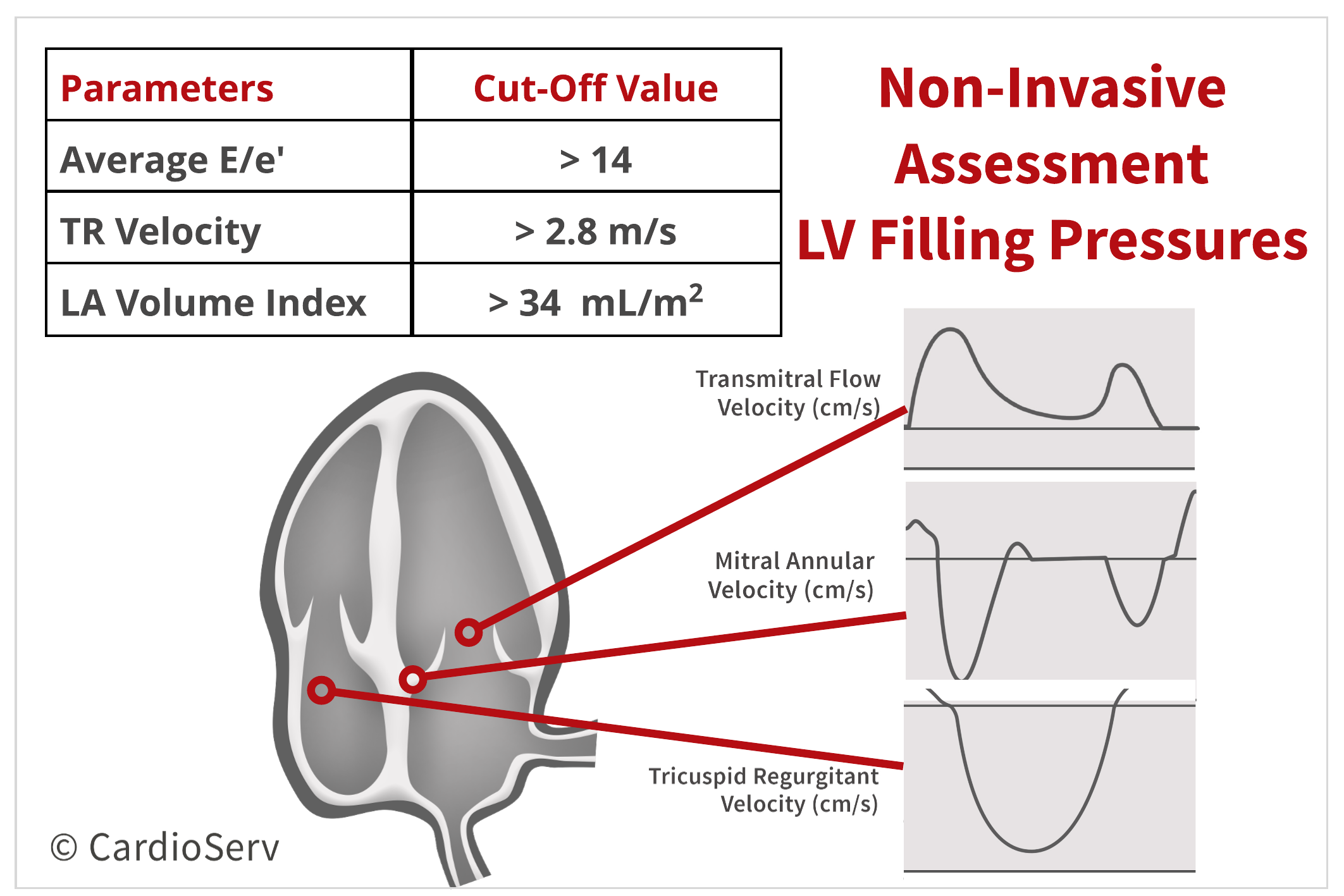
Echo can calculate this pressure by adding the peak systolic tricuspid regurgitation velocity and right atrial pressure (RAP). Refer back to our prior blog that explains how to obtain these values. A peak TR velocity > 2.8 m/s is suggestive of elevated LAP.
The transmitral pressure gradients (PG) determine the peak E-wave velocity, and can be used as an index for estimating LAP.
We are unable to take the peak E-wave velocity and transform it into a transmitral PG due to the true PG exceeding the predicted gradient with the Bernoulli’s equation. Therefore by measuring the peak E-wave velocity, which is the peak filling rate, we can correlate that value with the overall transmitral PG.
The LAP is the sum of the LV diastolic pressure and transmitral pressure difference. Therefore a limitation to using E-wave velocity as an index for LAP is the velocity reflects only the AV pressure difference. This is why we cannot use the peak E-wave velocity as the only parameter for determining the LAP.
The E/e’ ratio can be a useful parameter when used in combination of other measurements. A high E/e’ ratio is suggestive of elevated LVEDP. This method is useful because it is not effected by age and is a strong supporter of the presence of diastolic dysfunction. E/e’ ratio > 14 is considered abnormal.
The reason the E/e’ ratio is only useful in combination of other methods is due the wide normal range of the e’ value and specific limitations to e’.
By measuring the left atrium volume and indexing it to the patients BSA, it can provide valuable information about the LAP. As LV filling pressure progressively elevate, the LAVI size will enlarge. Therefore, an enlarged LAVI is a marker of elevated LAP. In contrast, a small or normal LAVI is suggestive of normal LAP. The abnormal cut-off value for LAVI is > 34mL/m².
This measurement is not an index of determining the LVEDP because the atrium will not enlarge immediately once pressures elevate. It’s also good to note, even when LVEDP become normalized, the size of the left atrium may continue to be enlarged. That is why we cannot use the LAVI size as a direct index of determining the LAP.
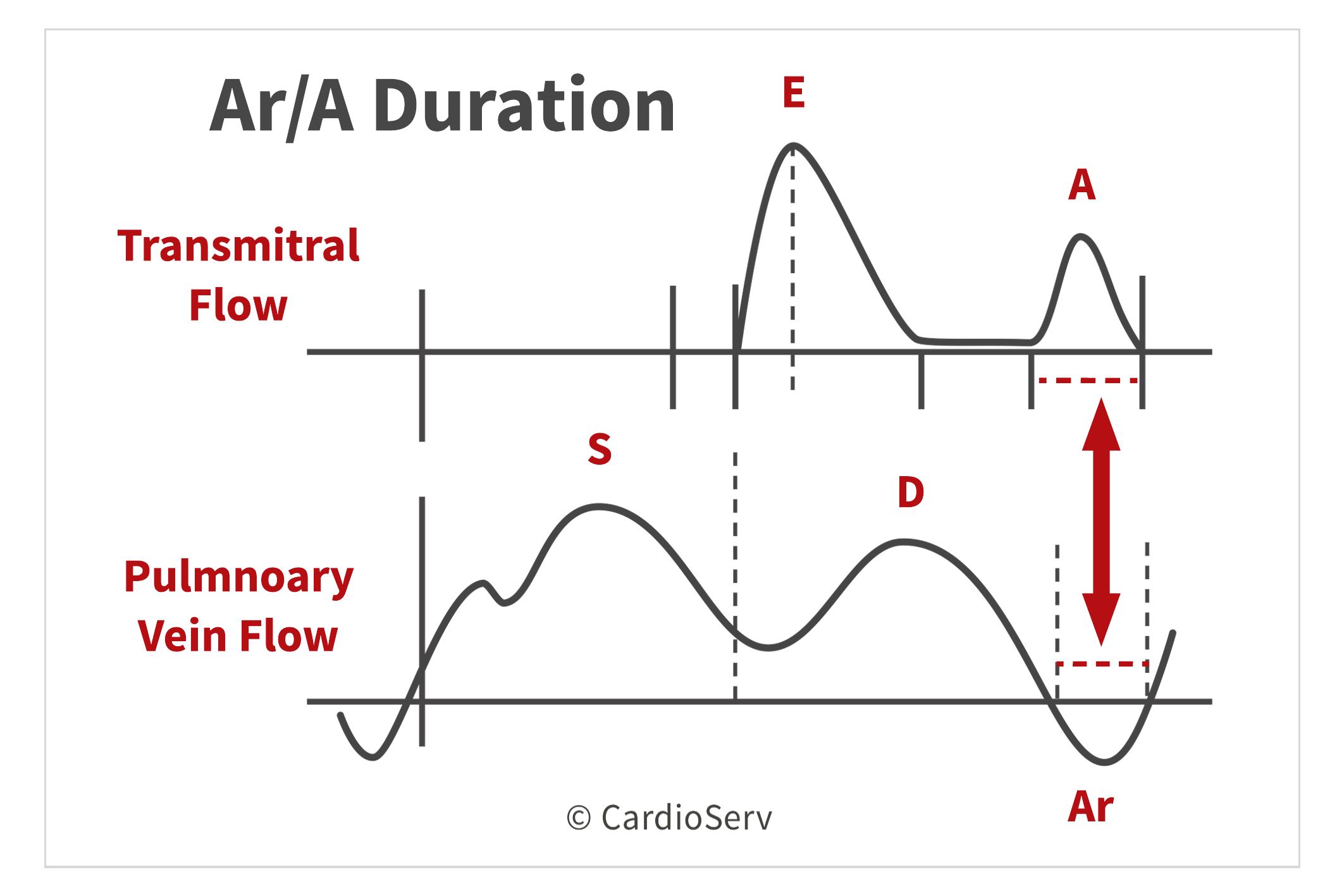
The comparison of time duration between the pulmonary venous antegrade Ar velocity and transmitral A-wave velocity can be used to estimate the LVEDP. An Ar/A duration> 30 ms is consistent with elevated LVEDP.
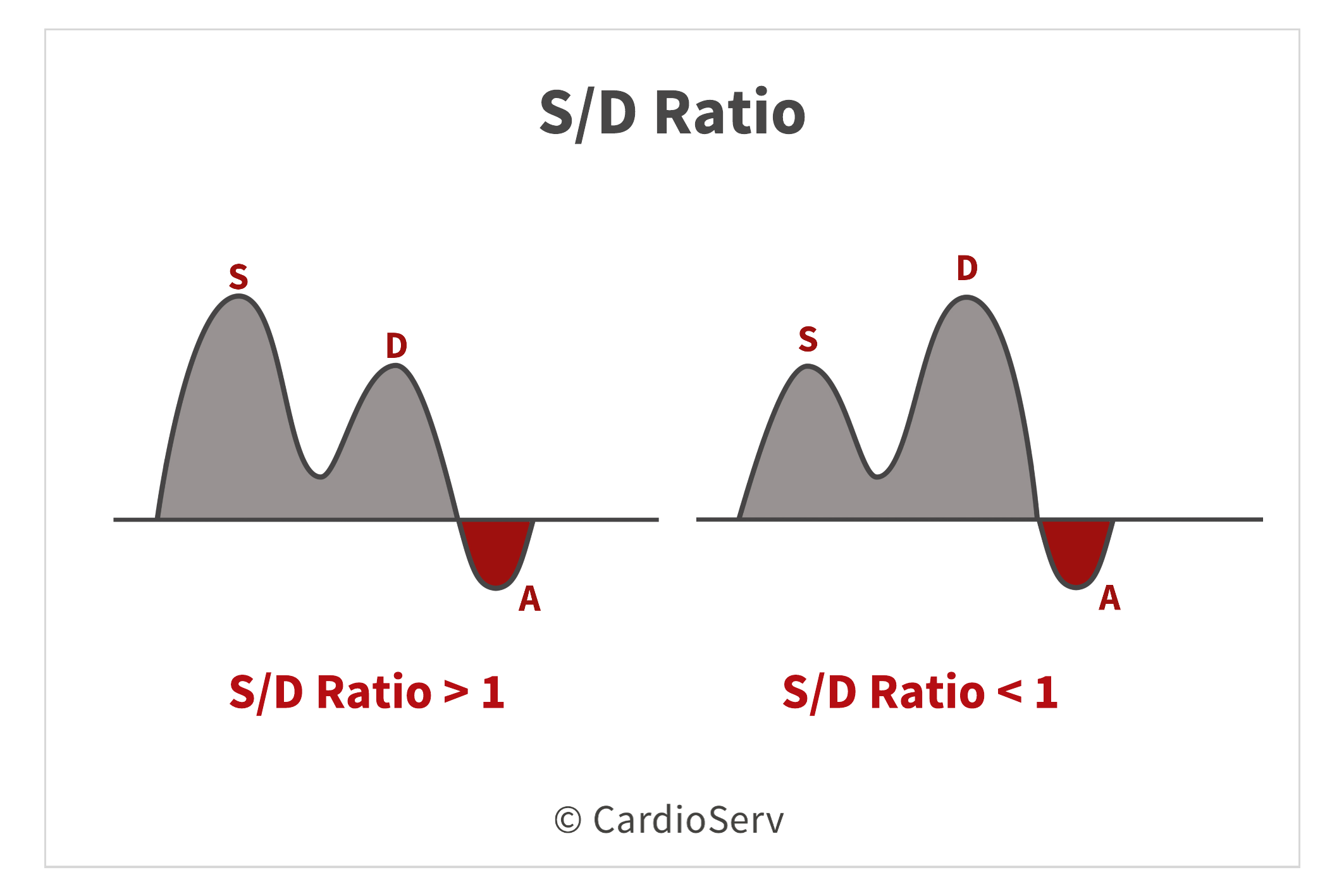
A S/D ratio < 1 can be used as an additional marker of elevated LAP in patients with depressed LV ejection fraction.
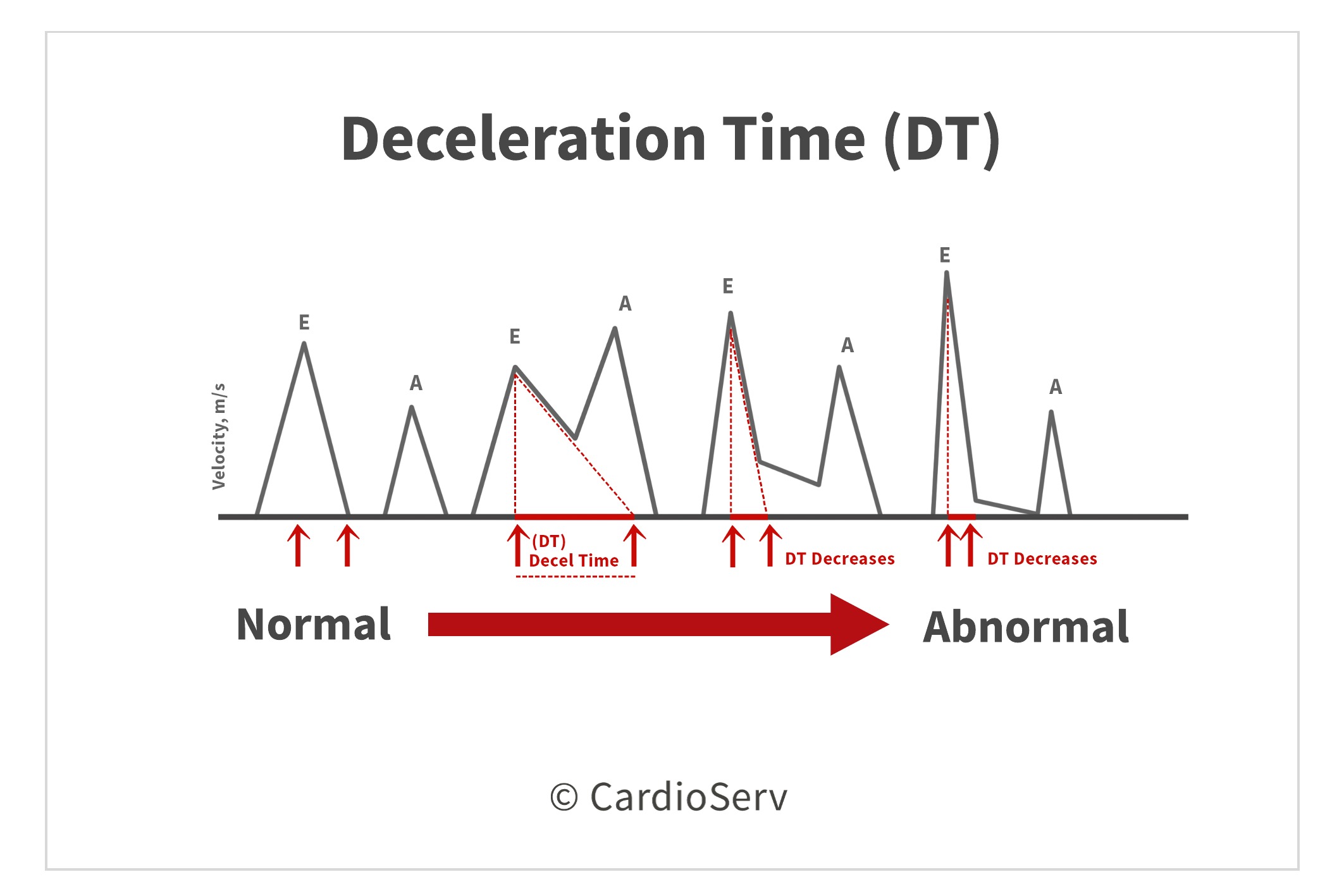
 Deceleration Time (DT)
Deceleration Time (DT)The deceleration time of the transmitral E-wave can be an additional tool because it reflects the ventricles relaxation and filling pressures. A short DT will be due to an increased E-wave velocity, which is caused by an elevated LAP.
 Other Parameters
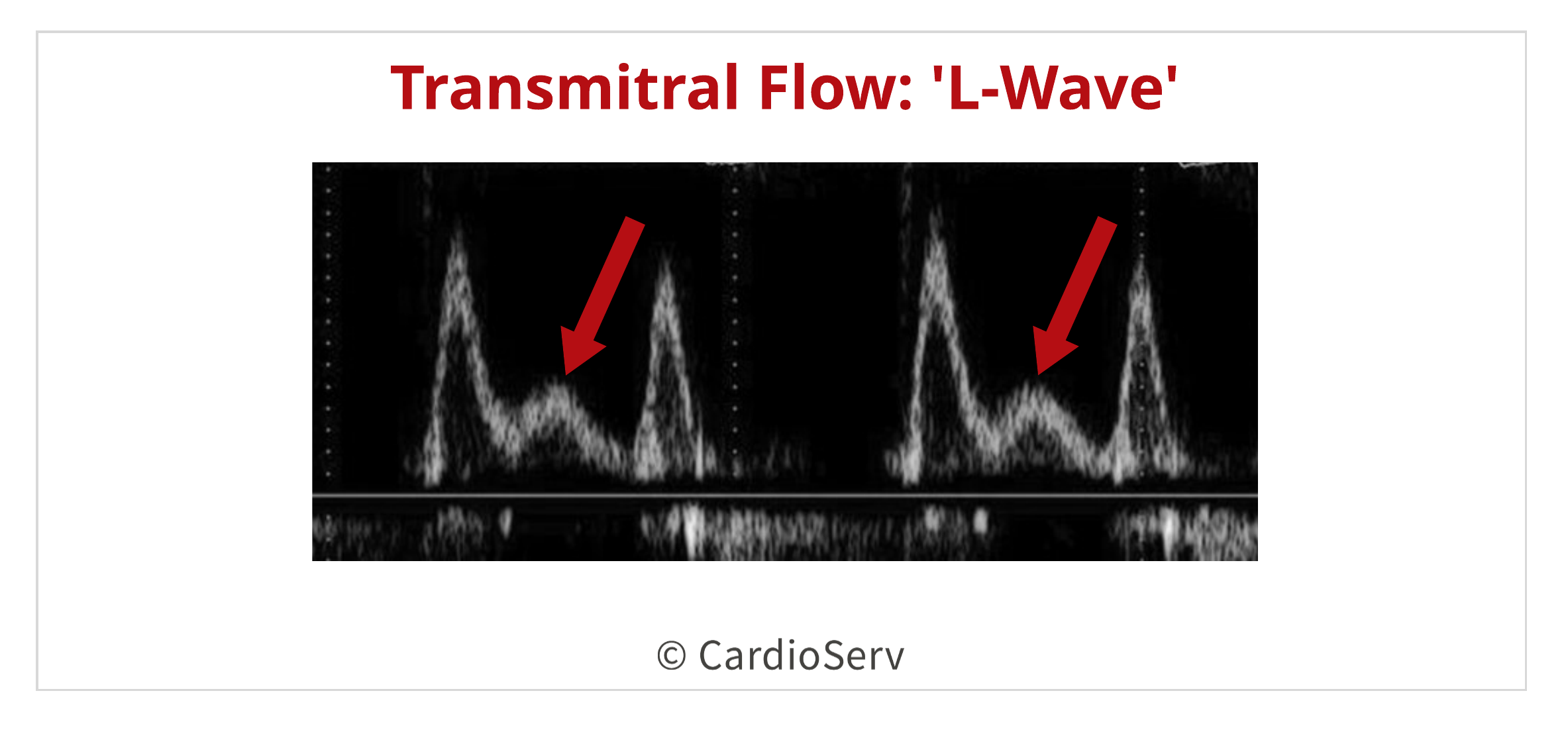
Other ParametersThe presence of a transmitral L-wave can be an additional sign of elevated LAP. The presences of this additional wave is caused by the pulmonary vein’s A-wave flow duration occurring longer into late diastole when there is impaired or prolonged LV relaxation present. This changes the normal biphasic transmitral flow into a triphasic display.
Another sign of an elevated LAP, is the delayed occurrence of the e’ velocity in comparison to the E-wave velocity. This delay in occurrence is telling us that the volume of blood is being pushed into the ventricle, instead of normally being pulled via a suction due to pressure gradient changes between chambers. This comparison is done when obtaining the E-wave and e’ velocity at the same time. Certain machines offer this feature of obtaining dual Doppler recordings simultaneously.
By using a combination of parameters, we can determine if the LAP is normal or elevated. It’s important to note that all parameters, except for estimation of TR velocity, must be used in combination and not as a single index for determining the LAP due to limitations for each measure.
The ASE provides two algorithms to use in conjunction with other indexes to determine both grade of diastolic dysfunction and presence of elevated LAP. Please refer back to our guest speaker blogs to view this information:
 Andrea Fields MHA, RDCS
Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Gillebert, T. C., Pauw, M. D., & Timmermans, F. (2013). Echo-Doppler Assessment of Diastole: Flow, Function and Hemodynamics. Education in Heart, 99, 55-64. Retrieved November 20, 2017, from https://pdfs.semanticscholar.org/deda/8ed40076f7bbb1da2668d190d15af9947c2d.pdf.
Nagueh, S. F., MD, Smiseth, O. A., MD, & Appleton, C. P., MD. (2016). Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and European Association of Cardiovascular Imaging. American Society of Echocardiography, 29(4), 277-314. Retrieved October 31, 2017, from http://asecho.org/wordpress/wp-content/uploads/2016/03/2016_LVDiastolicFunction.pdf
Andersen, O. S., MD, Smiseth, O. A., MD, & Dokanish, H., MD. (2017). Estimating Left Ventricular Filling Pressures by Echocardiography. Journal of the American College of Cardiology,69(15), 1937-1948. Retrieved November 29, 2017.
Mitter, S. S., MD, Shah, S. J., MD, & Thomas, J. D., MD. (2017). A Test in Content: E/A and E/e’ to Assess Diastolic Dysfunction and LV Filling Pressures. Journal of the American College of Cardiology,69(11), 1451-1464. Retrieved November 29, 2017.
Mottram, P. M., & Marwick, T. H. (2005). Assessment of Diastolic Function: What the General Cardiologist Needs to Know. Heart British Cardiovascular Journal,91, 681-695. doi:10.1136









Jan
2018
Sep
2020
Nov
2020