The ASE recently released their new 2017 valvular regurgitation updated guidelines back in April. The paper details the difference between primary and secondary mitral regurgitation (MR) and outlines proper evaluation methods for the most common pathologies seen. The past couple of weeks, we have discussed how to differentiate between primary vs. organic and acute vs. chronic. If you need to refresh or missed our blog, you can read them here:
This week the goal for our blog is to provide a clear & easy breakdown on how to evaluate different abnormalities of the mitral valve. We will review the Carpentier classification and how it relates to evaluation of the following abnormalities of the mitral valve:
Dr. Alain Carpentier is a french surgeon who developed the pathophysiological triad and Carpentier classification method for evaluation of mitral valve disease. This criteria chart is helpful for functional classification of mitral valve disease and is used by cardiologist and surgeons to aid with decision making on repair vs. replacement of the mitral valve.
Etiology is relevant to long-term prognosis, therefore placed at the top of the triangle. The bottom two corners (lesions and dysfunction) are relevant for treatment strategy.
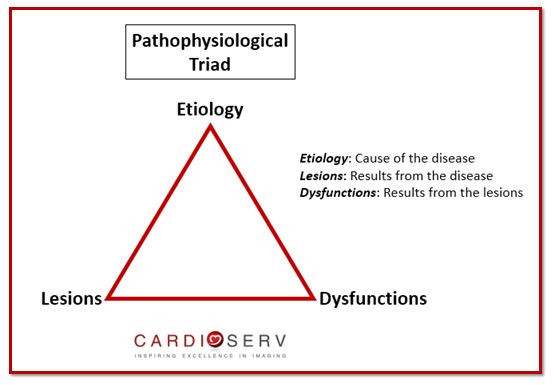
Examples include:
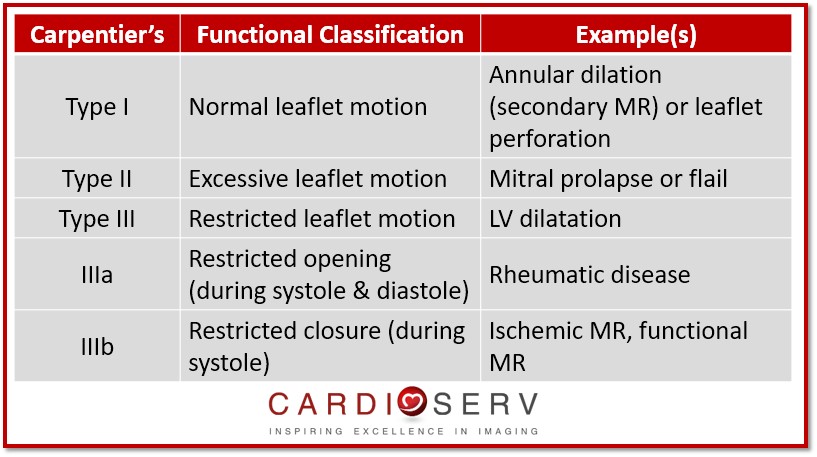
Let’s review Dr. Carpentier functional classification chart to describe the mechanism of the valve dysfunction, based upon opening & closing motions of leaflets.
Degenerative MV disease is the most common cause of primary MR. The two most common types of myxomatous degenerative MV disease include: fibroelastic deficiency & Barlow’s disease. Learn more about primary/organic MR in our recent MR mechanism blog.
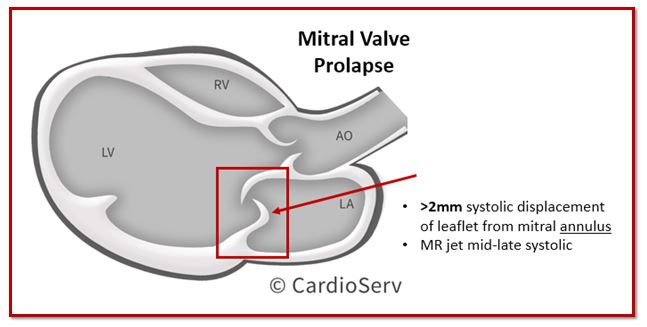
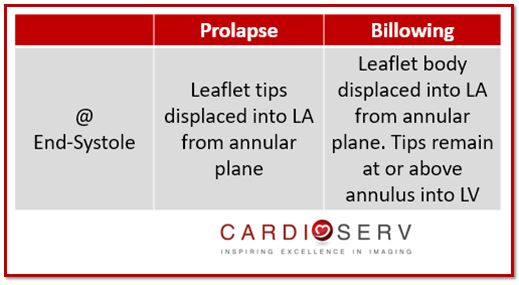
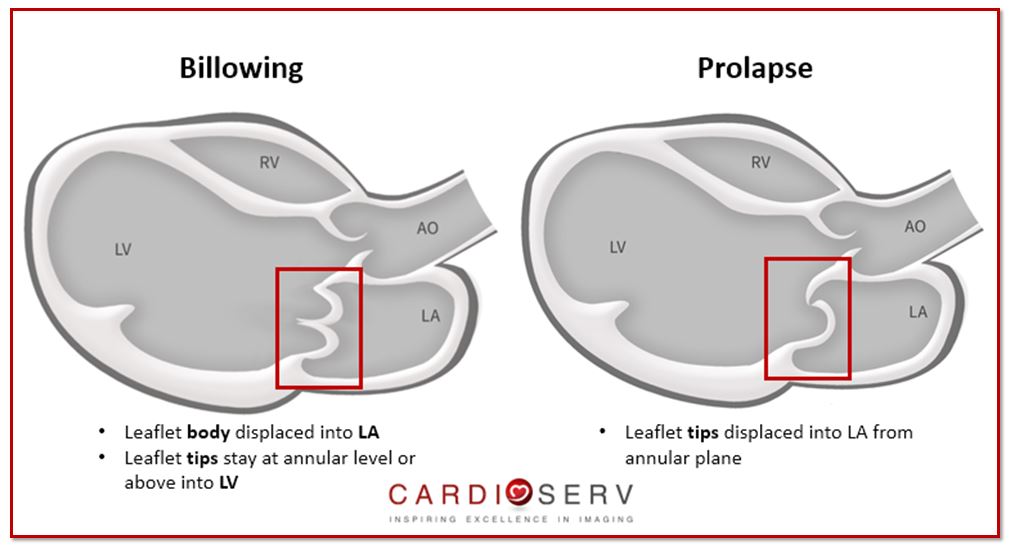
Mitral Valve Prolapse (MVP) is a type of primary myxomatous valve disease. This happens when there is a fibroelastic deficiency to a focal segment of the leaflet, causing a systolic displacement of the leaflet into the left atrium (LA).
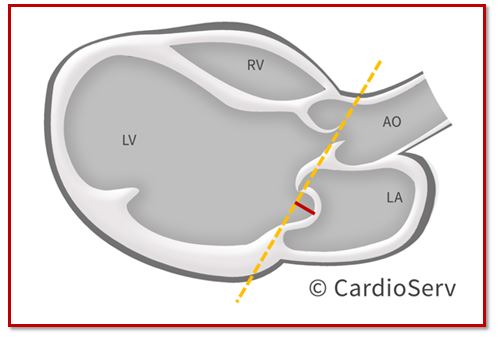
When evaluating the severity of MVP, it is suggested to do so in the parasternal long axis (PLAX) window. Apical 4 and 2 chamber windows are not ideal for diagnosing MVP due to the mitral annulus sitting too low, which can lead to a falsely displaced leaflets into the LA.
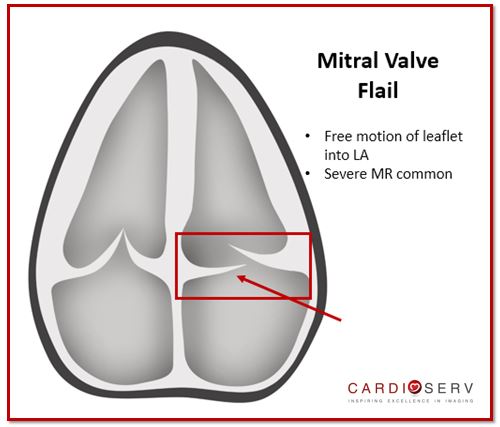
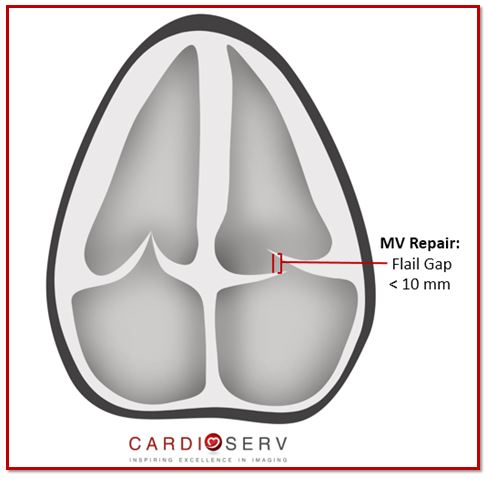
Flail Leaflet is when the leaflet edge and body have free motion into the LA, commonly due to rupture of chordae. It is usually always associated with severe regurgitation. In extreme cases, flail MV can be caused from papillary muscle rupture. Causes of rupture chordae can be due to:
Barlow’s Disease is an extreme case of MVP, due to an excessive amount of myxomatous tissue being present. Commonly both leaflets, (including multiple segments) become thick, bulky and redundant causing leaflets to ‘billow‘. In most cases, the mitral annulus will become dilated & enlarged and the chordae will be elongated.
This week we reviewed the Carpentier Triad and discussed how to properly identify and evaluate primary mitral valve disease, including:
As physicians, sonographers & healthcare clinicians–we need to remember the importance of identifying the mechanism & etiology that causes mitral regurgitation. They play a major role in the severity of the regurgitation, cardiac remodeling and management process of the patient. Stay tuned for the upcoming weeks to follow as we dig deeper into our mitral regurgitation blog series!
Our goal at CardioServ is to provide you with an easy process of understanding and properly evaluating mitral regurgitation! We look forward to hearing feedback and comments from our readers!
 Andrea Fields MHA, RDCS
Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Jouan, J. (2014). Mitral Valve Repair Over Five Decades. Annals of Cardiothoracic Surgery,4(4), 322-335. Retrieved July 6, 2017, from http://www.annalscts.com/article/view/6825/7706
Asgar, A. W., Mack, M. J., & Stone, G. W. (2015). Secondary Mitral Regurgitation in Heart Failure. Journal of the American College of Cardiology,65(12), 1231-1249. Retrieved July 6, 2017, from http://www.onlinejacc.org/content/65/12/1231?_ga=2.101757569.1871068379.1498150942-2075798501.1487771433
Saito, K., Okura, H., Watanabe, N., Obase, K., & Tamada, T. (2012). Influence of Chronic Tethering of Mitral Valve on Mitral Leaflet Size and Coaptation in Functional Mitral Regurgitation. Jour,5(4), 337-344. Retrieved July 6, 2017, from http://www.imaging.onlinejacc.org/content/5/4/337?_ga=2.169400609.1871068379.1498150942-2075798501.1487771433
Dal-Bianco, J. P., MD, Aikawa, E., MD, Bischoff, J., PhD, Guerrero, J. L., BS, & Hjortanes, J., MD. (2016). Myocardial Infarction Alters Adaptation of the Tethered Mitral Valve. Journal of the American College of Cardiology,67(3), 275-288. Retrieved July 6, 2017, from http://www.onlinejacc.org/content/67/3/275?_ga=2.126940813.1871068379.1498150942-2075798501.1487771433
Zoghbi, W. A., MD, FASE, & Adams, D., RCS, RDCS, FASE. (2017). Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation. JASE, 30, 4th ser., 1-69. Retrieved June 12, 2017.









Jul
2017
Aug
2017
Nov
2018