Last week we discussed the algorithm for determining the presence of diastolic function in patients with normal ejection fraction (EF). This week, we are going to discuss determining the presence of diastolic function in patients with depressed EF or pathologic left ventricular hypertrophy (LVH) with preserved EF.
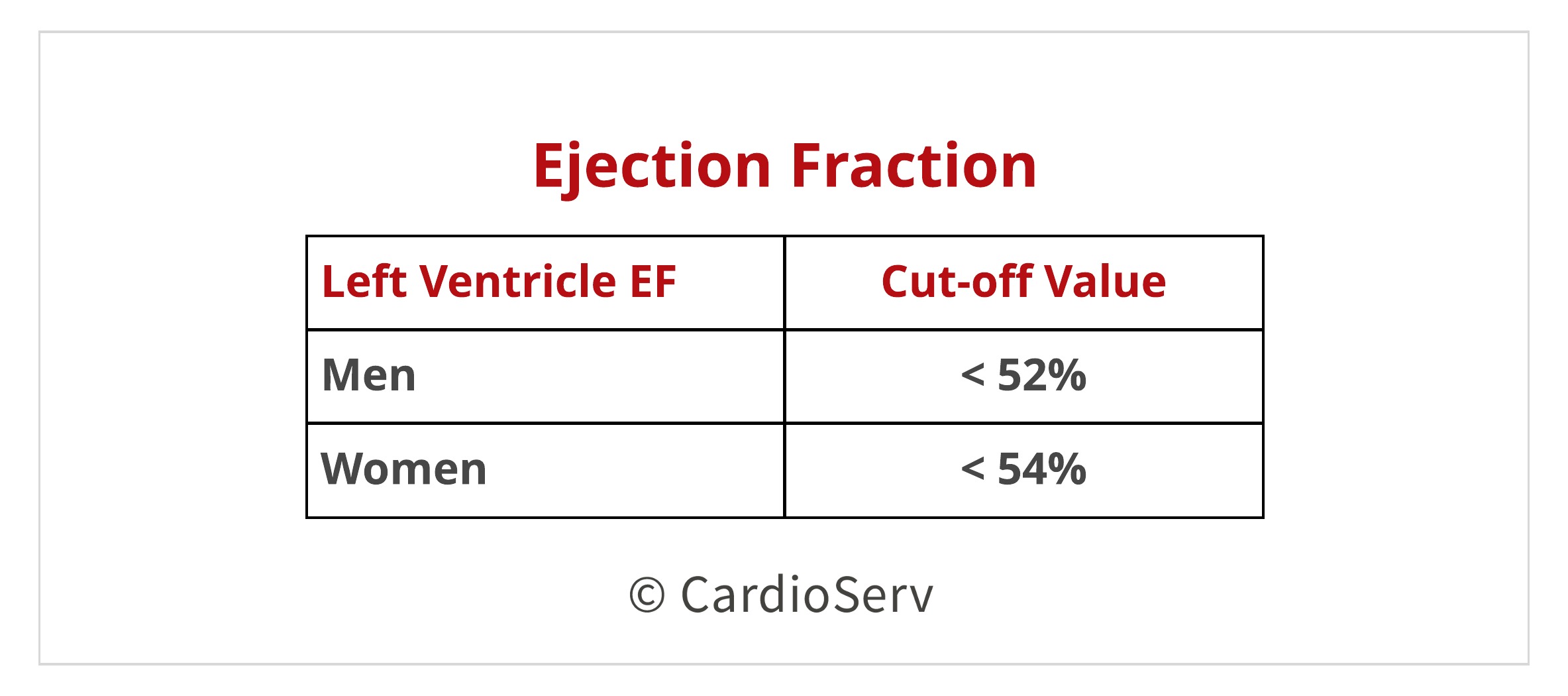
In order to determine the patients ejection fraction, the ASE suggest using the bi-plane volumetric method. You can check out CardioServ’s blog here that explains how to perform this measurement! ASE’s 2015 guidelines explain the cut-off values for LVEF:
The guidelines for this algorithm pathway also includes patients who have left ventricular hypertrophy (LVH) with a preserved ejection fraction. You can check out CardioServ’s blog here that covers how to determine the presence of LVH!
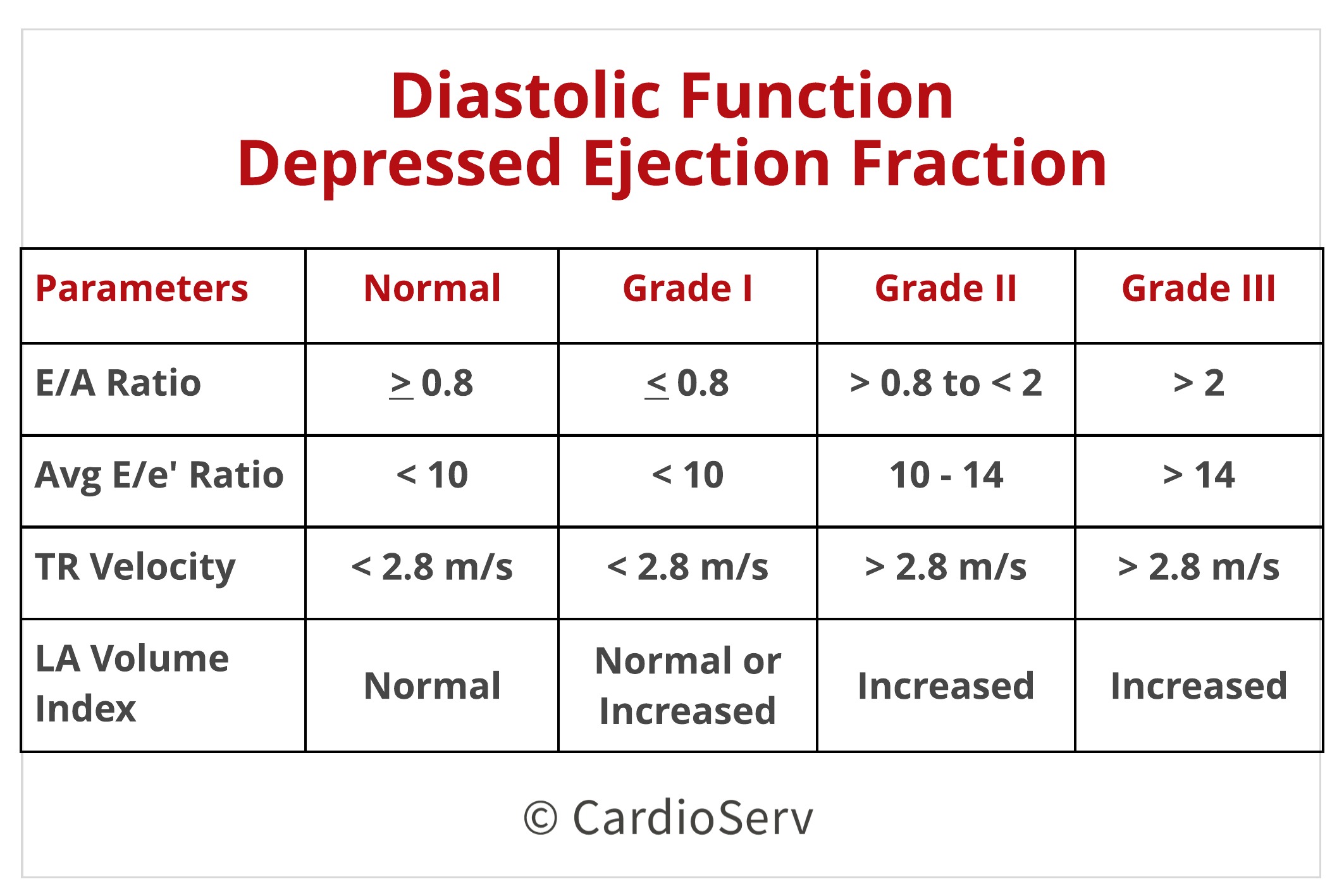
With this patient population we will place a heavier emphasis on the mitral E/A ratio. For this algorithm, we will be evaluating the following parameters:
You can check out our blog here to review how to acquire these measurements!
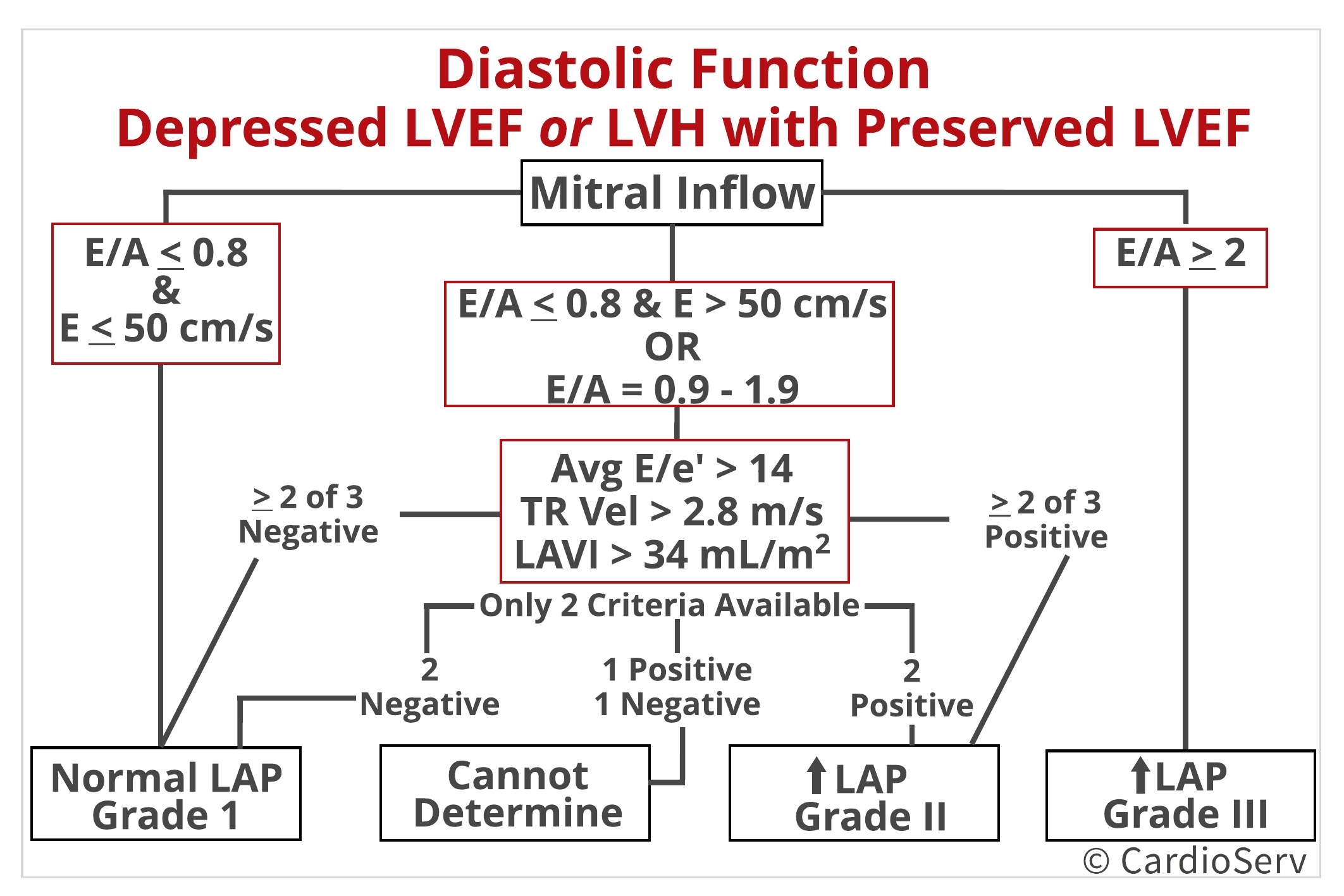
Let’s begin with the first step of the chart. There are three columns that dictate which grade of dysfunction you will eventually arrive at. First, evaluate where your E/A ratio falls.
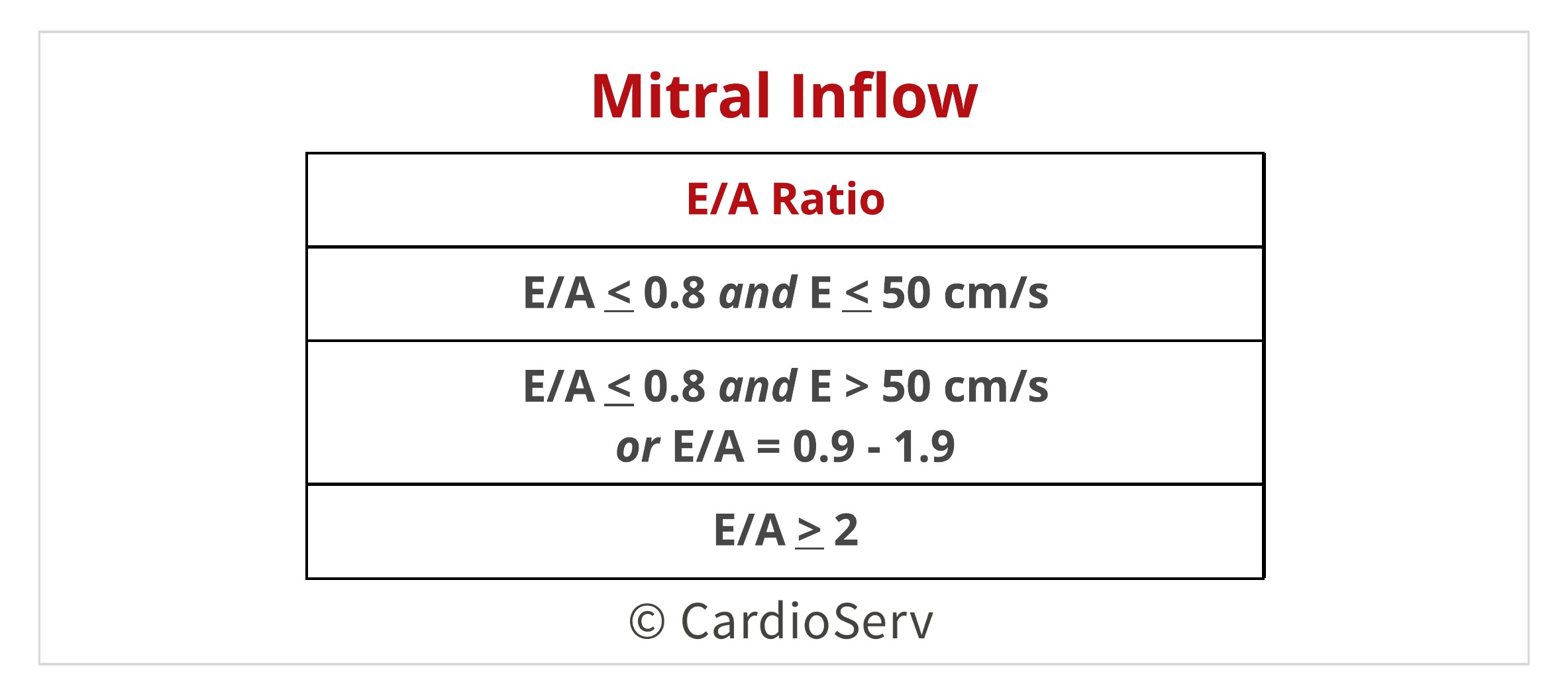
To keep things simple, let’s look at the first and third options
Here is where things get a little tricky: When your E/A ratio falls into the second category, there appears to be a slew of possibilities but it is actually quite simple. Let’s return to the above mentioned parameters that will be utilized after you move past E/A ratios and have landed into the second category.
Let’s recall the values associated with the parameters used for evaluating diastolic function:
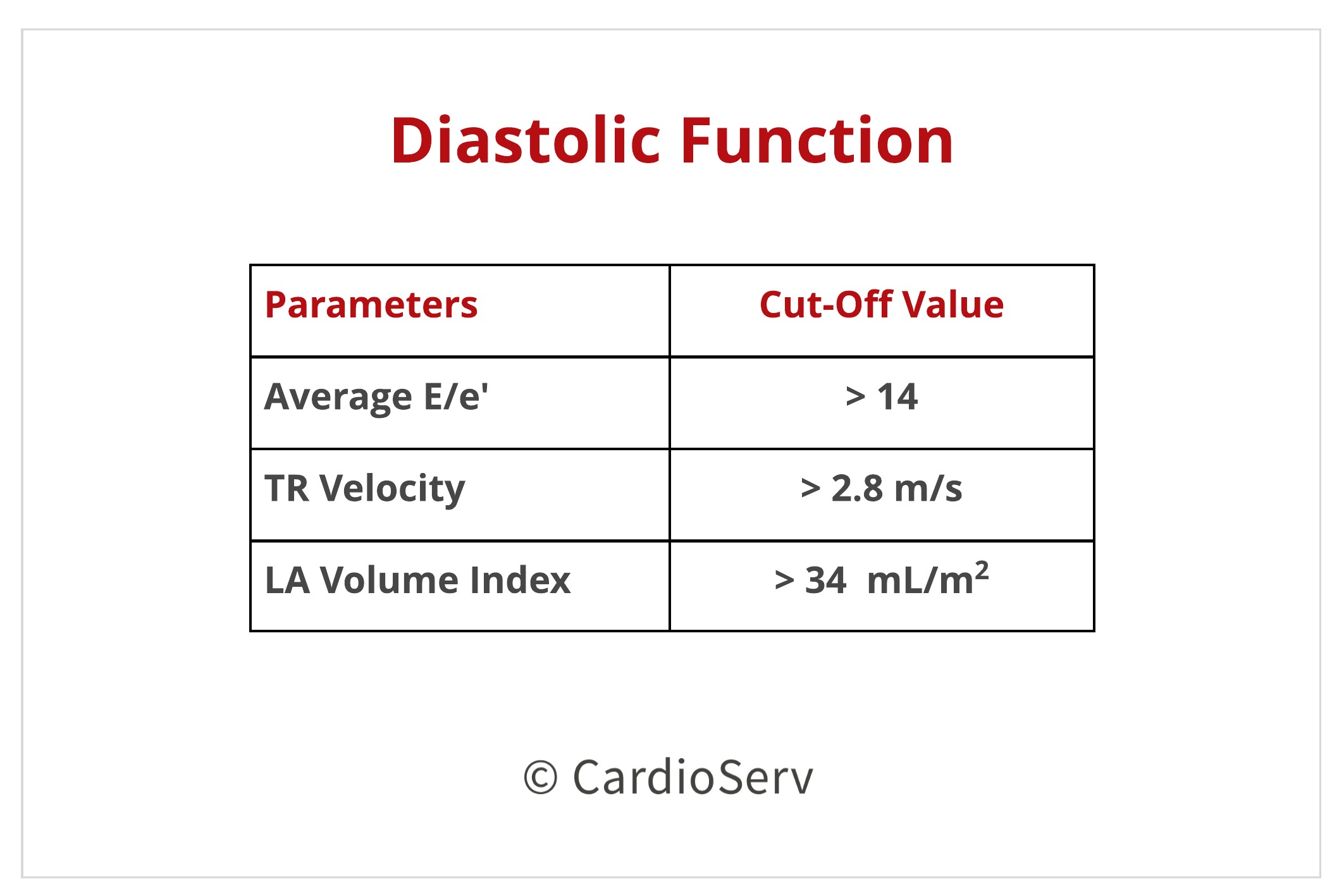
First, let’s assume you have properly obtained all 3 of these measurements. If this is the case, then:
Now, let’s assume that you did not have all three of the above mentioned parameters but rather only 2.
Lastly, if you only have one of the three measurements obtained, the pulmonary vein S/D ratio can conclude there is elevated LAP if the ratio is <1. As a reminder, this is to only be applied in patients with depressed EF.
Anytime you arrive at Grade I Dysfunction with Normal LAP and the patient is symptomatic, you MUST consider coronary artery disease (CAD) or proceed to diastolic stress testing.
We have now covered 2 algorithms for evaluation of diastolic function over the past two weeks. These workflow charts cover patients with normal ejection fraction, depressed ejection fraction and LVH with preserved ejection fraction. Next week we will cover how to evaluate diastolic function in patients with present abnormalities.
 Michael Owen RDCS, RVT
Michael Owen RDCS, RVT
Connect with Michael: LinkedIn, iEchoToday
Check out iEchoToday’s Facebook
If you need additional information on how to obtain correct diastolic measurements check out CardioServ’s recent blog on Correct Techniques to Acquire Diastology Measurements. This article reviews how-to obtain:









Nov
2017
Apr
2018
Nov
2017
Nov
2017
Nov
2017
Feb
2018
Mar
2018
Dec
2020