While vital for high-quality care, imaging accreditation can be challenging and sometimes tedious for imaging departments. To help, this article series offers some tips for how to comply with the latest Intersocietal Accreditation Commission (IAC) Quality Improvement (QI) requirements with quality and ease.
Part 1 and part 2 focused on the four required QI measures implemented by the IAC for all imaging modalities, which it separates into divisions for purposes of accreditation. The IAC is allowing each modality division one additional measure, which I like to call the “QI wild card.” We’ll focus on those additional measures in this article.
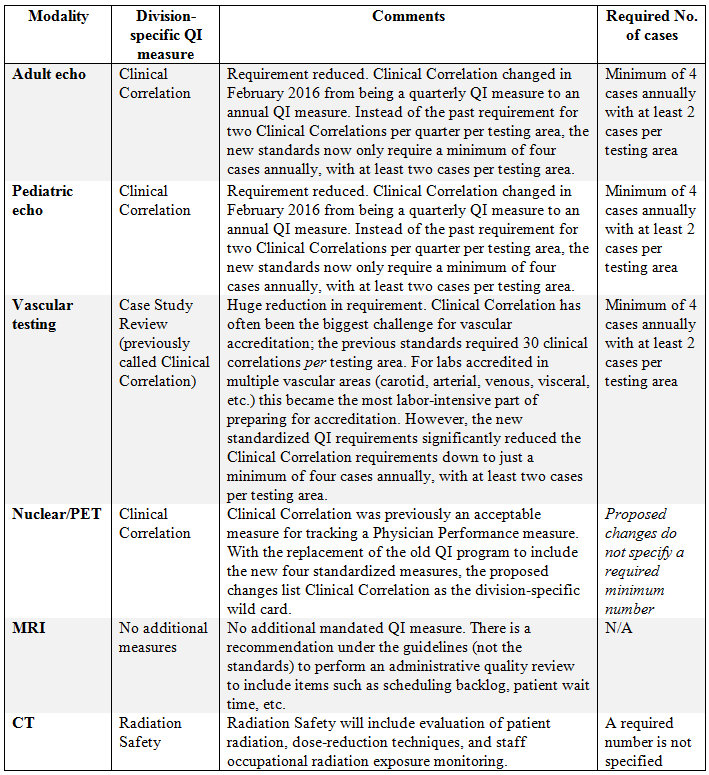
The MRI division chose not to add any additional mandated requirements. Instead, its guidelines include recommendations to perform an administrative quality review. This is not a mandate of the QI program, but rather a recommendation listed under guidelines. As for the other imaging modalities, CT added a new Radiation Safety measure. Nuclear added a Clinical Correlation measure as its wild card.
ECHO WILD CARD
The echocardiography division (adult and pediatric) chose to keep its Clinical Correlation measure as its wild card. When this became effective in February 2016, the Clinical Correlation measure was reduced in both the total number of required studies and the frequency of assessment. Clinical Correlation is no longer a quarterly measure; it’s now an annual measure. However, the total number of required cases has been reduced to a minimum of four cases annually, with at least two cases per testing area.
VASCULAR WILD CARD
The vascular testing division saw the most changes; IAC has redesigned the entire quality improvement program.. So is there good news somewhere here within the wild-card section? Oh yes! The vascular division chose a wild card it calls Case Study Review. This replaces the functionality of its Clinical Correlation measure but — this is where you hear the drum roll — with a massive reduction in the hard-to-get, pull-your-hair-out, “Are you kidding me?” past requirement of 30 clinical correlations per testing area.
Vascular reduced its required number of Clinical Correlations from 30 cases per testing area to just two! That’s not a typo. The exact standard reads like this: “Case review with any appropriate imaging modality, surgical findings, clinical outcome or other comparison of a minimum of four cases annually with at least two cases per relevant testing area (extracranial, intracranial, arterial, venous, visceral, screening).” Vascular sonographers can now rejoice in the ease of the clinical correlation that they will now breeze through!
QI DOCUMENTATION/MEETINGS
There’s a common phrase used regarding compliance: “If you didn’t document it, it didn’t happen!” Remember to document all of your QI findings. This documentation must be readily available to all staff. In addition, the staff needs to present the QI findings at one of your quality improvement meetings.
You can also keep your measures in a QI binder, post them in your department break room, or post on your hospital’s internal intranet that allows access to all staff members.
Following the theme of easing up on the burden of QI measures, the IAC standardized the number of required QI meetings to only two meetings per year. For echo and nuclear this was a welcomed reduction from the previously mandated four meetings annually. Here is a summary of the new, easier QI requirements:
- Two meetings per year
- All staff must attend at least one
- Staff must present the findings from the QI measures in at least one meeting
- The preference is for physical attendance, but remote attendance is allowed (via phone or internet)
- In a worst-case scenario when attendance is near impossible, staff can review the meeting minutes and sign off on them
Remember, there are still plenty of quarterly QI measures across the board. So don’t mess with a good thing if you have a system in place with your QI meetings to facilitate the completion of quarterly measures — specifically physician peer-review measures. The two meetings per year are assuming that staff completes all peer review quarterly. For facilities that don’t want to start assigning homework to the physicians, quarterly working meetings may still be the best option.
ACCREDITATION WITH QUALITY AND EASE
We’ve covered a lot of material so far in this accreditation series. Now that you know the four required measures in the new standardized QI program and the wild card, you understand the IAC’s expectations of your imaging department. With that as a foundation, we’ll turn our attention in future articles to time-saving techniques and tricks for completing each measure.
NEED HELP?
The staff members at the IAC are the nicest, most professional, and helpful group of individuals you could ever want to work with. Don’t be shy about reaching out to them for assistance. Also, check out the useful resources they provide on their website. They even offer sample documents for you to use in regard to both policies and QI forms.
In addition, feel free to reach out to us at CardioServ with any questions, and we will be happy to share our wealth of information and resources with you. I look forward to sharing tips and techniques throughout the rest of this series to ensure your success.