
Last Updated on January 30, 2024 by Hannes van der Merwe
While vital for high-quality care, accreditation can be challenging and sometimes tedious for imaging departments. To help, this series of articles offers some tips for how to comply with the latest Intersocietal Accreditation Commission (IAC) Quality Improvement (QI) requirements.
In part 1, part 2, and part 3 of our series, we reviewed the new IAC QI measures implemented across all imaging modalities:
- Test appropriateness
- Technical quality
- Interpretive quality
- Report completeness
- Wild card (modality-specific)
The remaining articles in the series will break down the QI measures into bite-sized tasks that everyone can perform. We will also offer time-saving tips, suggestions, and resources. Our goal at CardioServ is to allow you to focus on excellence and to practice at the highest possible level of quality.
JUMPING IN WITH REPORT COMPLETENESS
It can be challenging to start creating a compliant quality improvement program. Where do you begin? We recommend selecting report completeness as the first QI measure to work on. It’s the easiest to complete, and you’ll enjoy a sense of accomplishment as you check the first completed measure off your list!
This measure requires evaluating final reports for completeness and timeliness. All modalities must complete this measure, but only the echo (adult and pediatric) division specifies the required number of 10 reports. We suggest all modalities pull at least 10 reports per quarter in the early stages of assessing report completeness.
As you begin working to comply with the report completeness measure, we recommend breaking the task into two steps: gathering reports and completing the measure. You only need to pull 10 reports that you can quickly print and put to one side.
Here are five tips for pulling reports:
- Remember, the 10 reports need to represent all the testing areas in which you are seeking accreditation in your modality. For example, if you are seeking echo accreditation in the testing areas of echo, stress echo, and transesophageal echocardiography (TEE), you need to be sure that all of these tests are represented in your review. Vascular testing areas may include carotid, arterial, and venous studies, etc.
- Only pull a total of 10 reports, not 10 per testing area.
- Represent as many different reading physicians as possible.
- You can assign this task to anyone, including clinical and clerical staff or students.
- If you work alone, try printing reports while sitting at the reading station — first thing in the morning or at the end of the day. It doesn’t take long just to print the 10 reports; you will review them later.
THE RIGHT TOOL FOR THE JOB
Pulling 10 reports was an easy, quick step to get your feet wet with the QI program. Now what? The next step of report review can be just as painless with the right tool: a report checklist. This report completeness form should include a detailed list of each required item, not a generic form asking if all demographics, measurements, and report components are present.
As consultants, we automate this process through software, but prior to software development we created a line-by-line checklist for each modality. Imagine you’re holding a report in your hand (echo, vascular, nuclear, etc.) and I ask you if all the required demographics are included in the report. Could you answer immediately without knowing the IAC reporting standards?
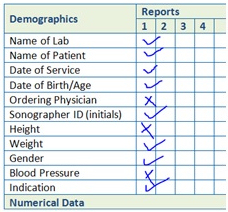
Now imagine, instead, if I ask you specific questions such as:
- Is the ordering physician listed?
- Are the patient’s height, weight, and gender included?
See how much easier that is? Imagine how that opens up the possibilities of who can complete this QI measure.
Here are four tips for creating time-saving report completeness forms:
- Pull out the guidelines just one time to create your original form(s). Once your form is finalized, you will not have to keep checking the standards over and over again.
- Include each and every reporting component in your form. Don’t generalize; be specific!
- Remember, it will be easier to assign this task to other members of the lab if you make this easy. For example, if your report should include left ventricular (LV) size and function, do not just list one line item that states “left ventricle.” Instead, list each specific part that you should be checking for on separate lines: LV size, LV function, and LV wall motion (if abnormal).
- Purchase ready-made forms or accreditation software.
NON-COMPLIANT REPORTS
So you have heeded our advice, broken the report completeness measure down into two steps, and created a report review checklist. You gathered your 10 reports one week and put them aside — in less than 15 minutes. The following week you used your new forms to complete your report review, and, again, you did this in less than 15 minutes!
Everything is going great, but wait — the reports are not compliant! This is expected with first-time accreditation. Even if you are an accredited lab, it’s common to find that reports sometimes start to slip a little after accreditation. No worries! Remember, the theory behind QI measures is that anything that is looked at gets better. You are already making progress toward improvement just by checking the reports for completeness and identifying areas that are missing.
DON’T IGNORE DEFICIENCIES
The point of any QI measure is to identify areas for improvement. It’s OK to identify these areas; it’s just not helpful to ignore them! Here are three tips to help improve report completeness:
- Post the report completeness checklist at the reading station so the reading physician can clearly see it.
- Make sure your reporting templates include areas to report on each component. This makes it easier for the physicians to be compliant:
- Set up fields on the reading stations for each required component.
- Even if your doctor is still dictating findings, he or she is using some kind of guide, most likely your worksheet. Update your worksheet to include all of the necessary demographics and report components.
- If the transcriptionist also receives the worksheet, there is no need for the doctor to dictate all of the demographics (height, weight, and blood pressure). All of that information will be on your worksheet.
- Whether your worksheet is a physical piece of paper or the electronic worksheet on a reading station, you can help the interpreting physician by providing your comments and observations for each required component.
GETTING HELP
In part 5 of our series, we will review another required QI measure and share our time-saving tips. Remember, the IAC is always happy to answer questions and they provide a wealth of resources on their website. In addition, our team at CardioServ is always just a phone call away. Feel free to give us a call, schedule a free consultation, or follow us on social media.




