Last Updated on January 12, 2026 by Don Gerig, RDCS
This week we are pleased to introduce our guest writer, Dr. Sukhvinder Singh. He will discuss the role of echocardiography in the presence of Left Bundle Branch Block.
Dr. Singh is a board certified cardiologist in India with 10 years of experience. He has worked at St. Stephen Hospital and Delhi Heart and Lung Institute and sits on the editorial board of many journals including International Journal of Diagnostic Imaging and Indian Journal of Cardiobiology and Clinical Sciences.
He is Review Board Member for cardiology and cardiovascular sciences for many international journals including BMJ group. He has a book chapter and more than 15 papers in various national and international journals to his credit. His key areas of interest are Tele-cardiology, preventive cardiology, echocardiography, stress testing and non-interventional cardiology. Dr. Singh currently runs a tele-cardiology web portal www.telecardiologyindia.com.
How Left Bundle Branch Block (LBBB) Affects Echocardiography

Regional wall motion abnormalities are a common abnormality encountered by cardiac sonographers and interpreters. Regional wall motion abnormalities are often easier to recognize in clinical circumstances suggestive of coronary artery disease (CAD) versus non-coronary scenarios.
Some reasons for non-coronary wall motion abnormalities being difficult to distinguish are because they are uncommon and less discussed, thus decreasing our experience with them. One such abnormality is Left Bundle Branch Block (LBBB). LBBB produces a wall motion abnormality that may mimic ischemic wall motion abnormality of the interventricular septum. Therefore, it is important for careful evaluation of wall motion in the presence of LBBB.
What is Left Bundle Branch Block (LBBB)?
LBBB is a common conduction disorder that may be present with or without any structural heart disease. LBBB is identified on ECG by the following criteria.
- QRS Duration more than 120 ms
- M or M’ pattern in V5/6 , I, AvL
- Loss of septal Q in I, V5-6 (except aVL)
- Secondary ST/T changes
- Ventricular activation time more than 60 ms in V5-6
- Loss of R in V1-3
Typical Wall Motion Abnormalities in LBBB on Echo
LBBB produces a wall motion abnormality that may mimic ischemic wall motion abnormality of interventricular septum. With careful evaluation of wall motion in the presence of LBBB, we can identify signs that help us to better differentiate ischemic wall motion abnormalities from LBBB.
The normal motion of interventricular septum (IVS):
- Systole: Continuous motion of IVS towards the center of LV
- Diastole: Backward motion, which takes place away from center of the LV
The Classically Described 2D Wall Motion Abnormality Due To LBBB
- Seen in all views of the septum (parasternal long, short and apical views)
- Early systolic movement of IVS towards the center of LV followed by movement away from the center of LV (paradoxical movement).
- The duration of this paradoxical movement is variable:
- It may be transient to almost complete duration of systole
- The longer the duration of this paradoxical motion, the more it appears to our eyes as a pathological regional wall motion abnormality
- Despite this paradoxical wall motion, there will be definite wall thickening of the IVS
- This wall thickening is the most important parameter, which helps in differentiating a viable from a non-viable septum. Presence of thickening also rules out a viable but ischemic & akinetic septum (hibernating myocardium).
- In some subjects, paradoxical movement is so transient that it appears only as a small jerk in the inward journey of septum towards center of LV
- While in others, it appears as complete dyskinetic movement of the IVS away from LV but with preserved myocardial thickening
- Wall motion abnormality due to LBBB is restricted to basal and mid part of IVS and it does not affect apical segments
- It may be helpful to review the 2D cine-loops in slow-motion
M-Mode Echo Findings in LBBB
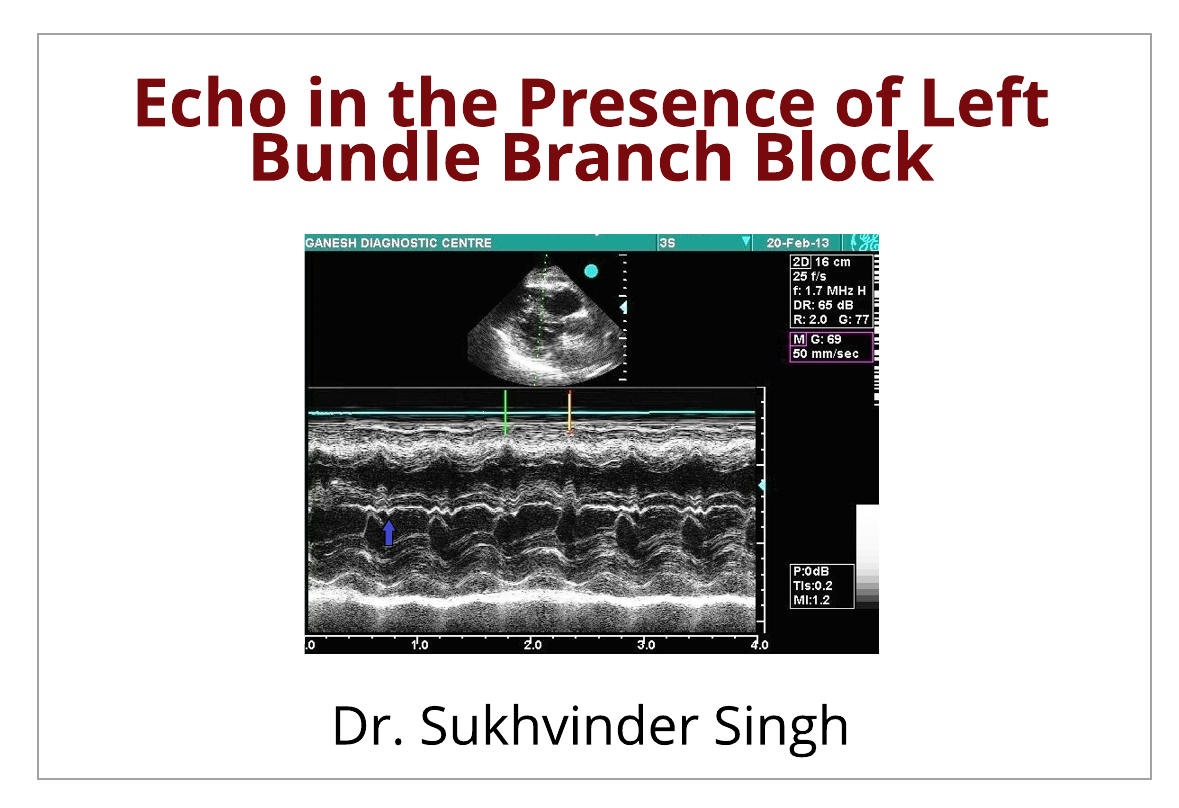
In all cases of LBBB it is important to record M-Mode through the anterior septum and the Mitral valve in Parasternal Long Axis (PLAX) with ECG gating. There is a beak like projection of IVS in M-mode in early systole
- This “beak” on M-mode tracing is produced as a result of movement of the IVS towards the center of the LV in early systole and followed by immediate backward retraction away from center of LV.
- This beak is seen just after the inscription of peak R wave on ECG or just at the closing of mitral valve.
Below Figure 1 – Red Arrow

Below Figure 2 – Purple Arrow

Temporal Dyssynchrony
Besides these characteristic finding, there may be inter-segmental temporal dys-synchrony in the left ventricle that may not always be apparent to eyes in every case. What is temporal dyssynchrony? This simply means that some of the LV segments contract later than other segments of the LV. In a normal LV, all segments tend to contract simultaneously. With LBBB there is an increase of total time taken to activate the left ventricle (increased QRS duration) and the inferolateral and anterolateral segments contract later than the other segments.
Cases of LBBB In Echocardiography
Let’s review some video images and pay specific attention to the motion of the anterolateral and inferolateral wall segments.
- These segments are contracting later as compared to inferoseptal and anteroseptal segments.
- We can see how the mid inferoseptal segment moves away from the center of the LV in systole while the apical-septal segment is moving inward.
- There is no thinning of any of the segments
LBBB in Parasternal Short Axis of the LV
LBBB- Apical 4 Chamber
LBBB- Apical 4 Chamber
Summary
In patients presenting with symptoms suggestive of CAD, echocardiographic conclusion that wall motion is explained by LBBB only is not sufficient to close the case. However, in those cases where patients are asymptomatic or have symptoms of some other disease (Non-CAD), a conclusion that the wall motion abnormality is due to LBBB only, helps clinicians to make the correct interpretation.
5 Characteristics That a Wall Motion Abnormality Is Due To LBBB:
- Early systolic beaking of IVS followed by transient or prolonged paradoxical motion
- Preserved wall thickening of IVS
- The wall motion abnormality will be restricted to basal and mid segments and will not extend to apical segments.
- Intersegmental temporal dys-synchrony
- No area of wall thinning
Dr. Singh currently runs a telecardiology web portal www.telecardiologyindia.com
Suggested reading
1. Dillon JC, Chang S, Feingenbaum H. Echocardiographic manifestations of Left bundle branch block. Circulation (May 1974). Vol 49. 876-80.
By: Sukhvinder Singh, MD, DM (Cardiology). www.telecardiologyindia.com




