Last Updated on January 30, 2024 by Hannes van der Merwe
CardioServ is dedicating the month of April to right heart quantification awareness! This month we will present a series of blogs to review the proper methods to quantify right ventricular size and function.
The right heart has jokingly been referred to as the step-child of the heart with often little attention paid to the size, function and prognostic implications of right heart findings. Over the years, ASE had written papers on the right heart that often had conflicting information and reference ranges. In 2015, ASE released the updated ‘Chamber Quantification Guidelines’ that included a detailed description on the right heart to replace past conflicting information.
This week we will review:
1. ASE general recommendation updates for right heart
2. How to perform a comprehensive 2D assessment of the right heart
3. Correct imaging windows to visualize the RV
4. Tips to better visualize the RV
ASE GENERAL RECOMMENDATIONS UPDATED
- All studies should include a comprehensive examination of the RV & RA.
- The echo report should include both qualitative and quantitative parameters for right heart assessment.
- RV & RA Size
- RV Systolic Function (via one or combination of the following)
- Fractional Area Change (FAC)
- TAPSE
- S’ Wave
- RIMP
- RV Systolic Pressure
- Tricuspid Regurgitation (TR) Jet
- Estimated Right Atrial Pressure (RAP)
- Based upon Inferior Vena Cava (IVC) Size & Collapsibility
- Abnormal cutoff values were changed for: RV Dimensions, S’ Wave, TAPSE and RIMP.
COMPREHENSIVE ASSESSMENT OF RV
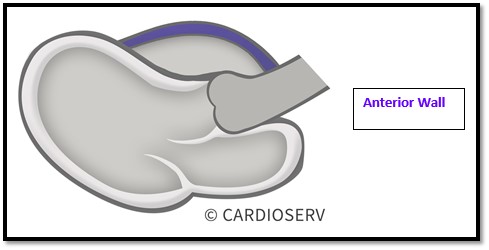
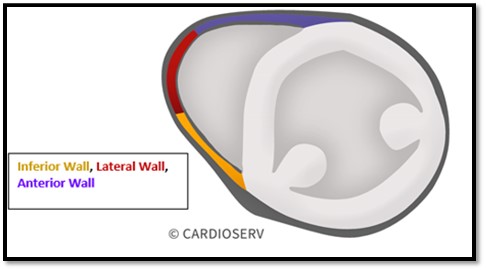
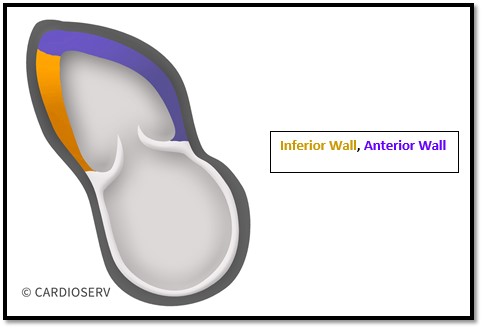
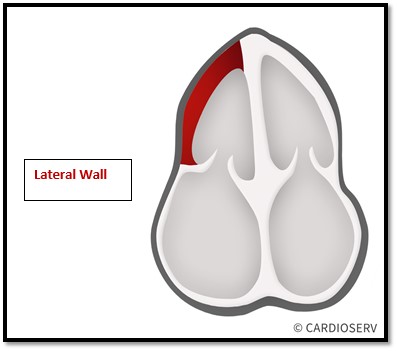
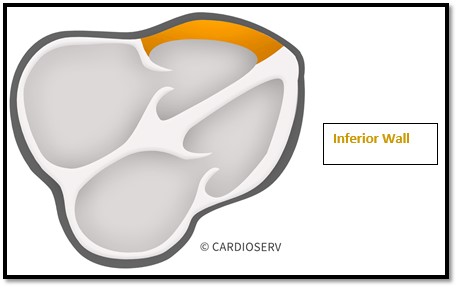
The RV has 3 wall segments, which include:
- Anterior Wall
- Inferior Wall
- Lateral Wall
There are 5 imaging views required to obtain, in order to properly evaluate all segments of the RV.
- Parasternal Long Axis (PLAX)
- Parasternal Short Axis (PSAX)
- RV Inflow Tract (RVIT)
- Apical 4 Chamber
- Subcostal 4 Chamber
IMAGING WINDOWS
WHY IS THE RV SO HARD TO IMAGE?!
The RV is the most anterior portion of the heart within the thorax, ending up in our near field of the ultrasound beam—which causes limited scanning windows and poor resolution.
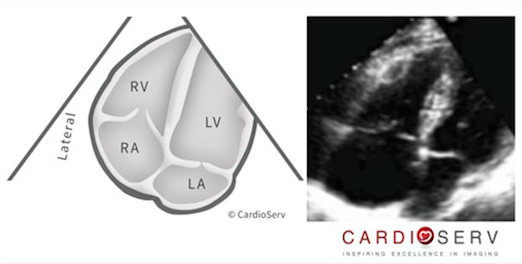
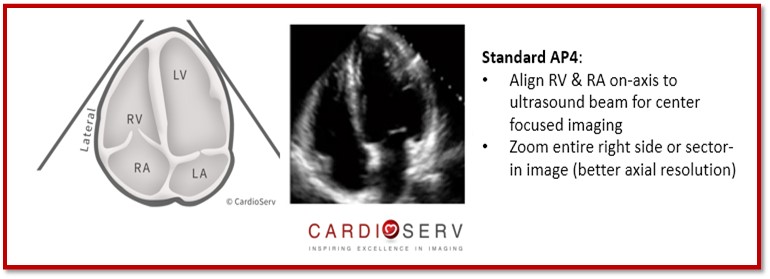
The ASE explained 3 different scanning views we can obtain from the AP4 window to properly quantify the RV & RA.
- Standard AP4
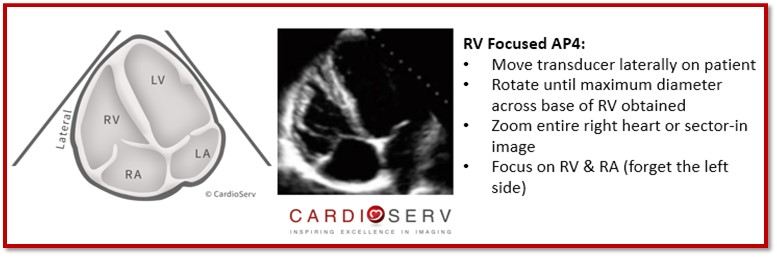
- RV Focused AP4
- RV Modified AP4
Standard AP4:
RV Focused AP4:
RV Modified AP4:
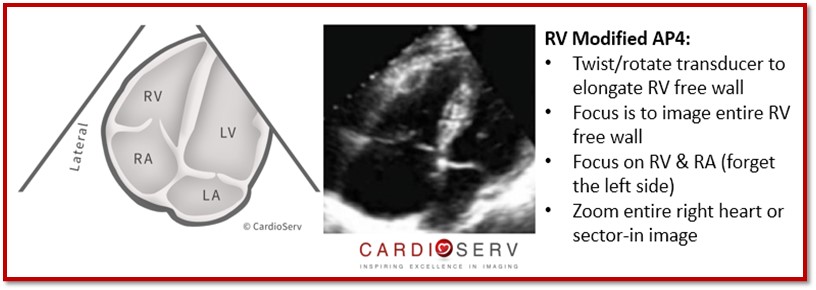
**Note: Quantitative methods should not be measured in this view. The purpose of this view is to qualitatively evaluate function of RV.
HOW CAN I BETTER VISUALIZE THE RV WITH DIFFICULT/LIMITED PATIENTS?!
There are a few techniques if we are having difficulty visualizing the RV:
- Change the angle of the transducer!
- Try to go more lateral or move up/down a rib space!
- Push IV Saline! (Just as you would for a Bubble Study)
- Help facilitate visualization of RV, but only last a few seconds.
- IV Echo Contrast (Just as you would for using it for LV Endocardium)
- It requires slower injection to prevent attenuation artifact.
CONCLUSION
We should now have a better understanding of:
- Reasoning for updated for right heart chamber quantification from ASE
- Basic RV wall segment review
- Specific imaging windows to obtain for evaluation of right heart
The goal of this blog was to review the recommendations from ASE regarding right heart assessment and to lay the foundation for the basics of correct right heart visualization. We will use the material we learned today and apply it further in our upcoming blogs that will discuss in detail the correct methods for right heart size and function quantification. Next week, for the right heart blog series, we are going to discuss the proper way of measuring the RV.

Andrea Fields, MHA, RDCS, Clinical Cardiac Director
References
Lang, R. M., MD, Badano, L. P., MD, & Mor-Avi, V., PhD. (2015). Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. JASE, 28(1), 1-53. Retrieved March 1, 2017, from http://asecho.org/wordpress/wp-content/uploads/2015/01/ChamberQuantification2015.pdf




