
Last Updated on March 16, 2026 by Don Gerig, RDCS
We dedicated the month of April to learning about ways to implement right heart quantification into our routine exams. This month, we are going to continue that journey and discuss ways to evaluate the function of the right heart!
“RV systolic function should be assessed by at least one or combination of the following: FAC, S’ Wave, TAPSE or RIMP.” –ASE JASE 2015
With that in mind, let’s jump into how to perform these!
ASE Guidelines for Assessing RV Systolic Function
The American Society of Echocardiography (ASE) recommends assessing right ventricular (RV) systolic function using a multiparametric approach. Commonly used quantitative methods include:
- TAPSE (Tricuspid Annular Plane Systolic Excursion)
- S’ Wave (Tissue Doppler Imaging of the tricuspid annulus)
- FAC (Fractional Area Change)
- RIMP (Right Ventricular Index of Myocardial Performance)
- RV Free Wall Longitudinal Strain – 2D Speckle Tracking (when available)
- 3D RVEF – 3D Right Ventricular Ejection Fraction (preferred when feasible)
These parameters offer complementary insights, and using more than one is encouraged to improve diagnostic accuracy.
In this article we’re going to discuss how to perform TAPSE & S’ Wave measurements.
With the release of the 2025 ASE Right Heart Guidelines, we’ve move beyond simple “normal” and “abnormal” cutoffs. Most parameters now include graded severity ranges of mild, moderate, and severe dysfunction. These values aren’t indexed to BSA, height, or gender but offer standardized reference ranges for greater consistency across labs.
Imaging Window For Evaluating RV Function
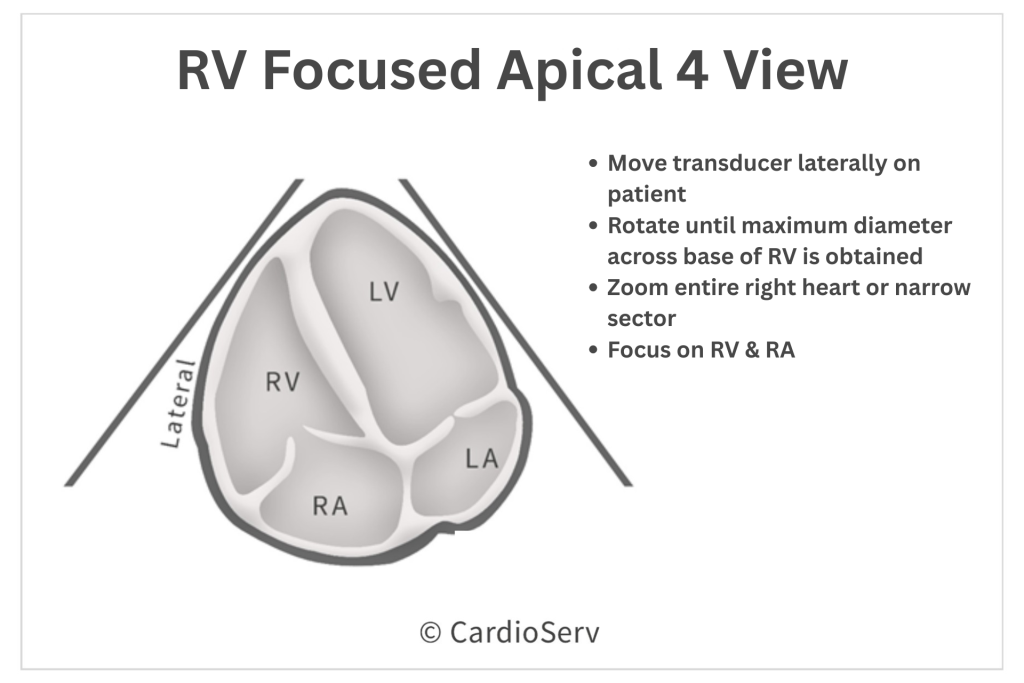
The ASE suggest using the RV focused Apical 4 Chamber window when performing an assessment of the right ventricle.
RV Focused Apical 4 Chamber (AP4)
How to Measure TAPSE & S’ Wave in Echocardiography
TAPSE: Tricuspid Annular Plane Systolic Excursion
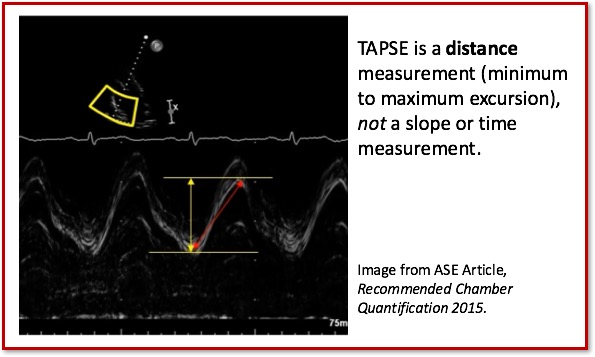
TAPSE is a linear M-Mode measurement of the RV longitudinal function.
- Wide Spread
- Established Prognostic Value
- Validated with Global RV Function
How to Perform TAPSE Measurement
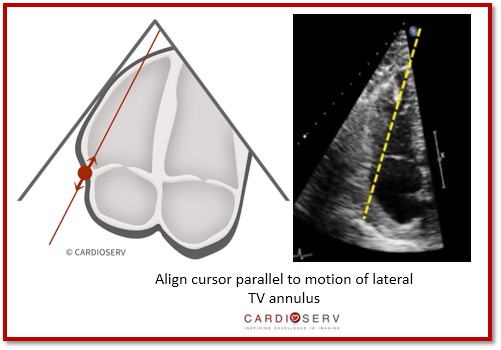
- Align M-Mode cursor parallel to motion of lateral TV annulus**
- Annulus should be moving upwards towards the apex during systole
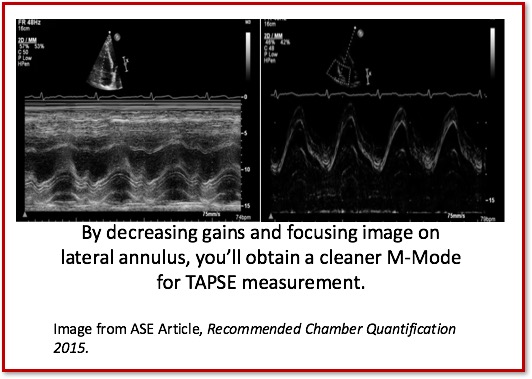
- Decrease gains to avoid measuring ‘noise artifact’
- M-Mode Speed: Medium-Fast
- Look for a consistent signal throughout systole and diastole
- Identify maximum systolic and diastolic excursion of annulus motion
- Measure VERTICALLY via leading-edge to leading-edge method
Challenges and Limitations to Linear Measurement
- Angle dependency: Even small misalignment can significantly underestimate true motion.
- Load sensitivity: Changes in preload or afterload can affect TAPSE adn S’ wave.
- Regional limitation: These parameters reflect only basal longitudinal motion, not global RV performance.
- Over- or underestimation risk: Common in conditions such as severe TR, post-surgical RV distortion, or pacing leads.
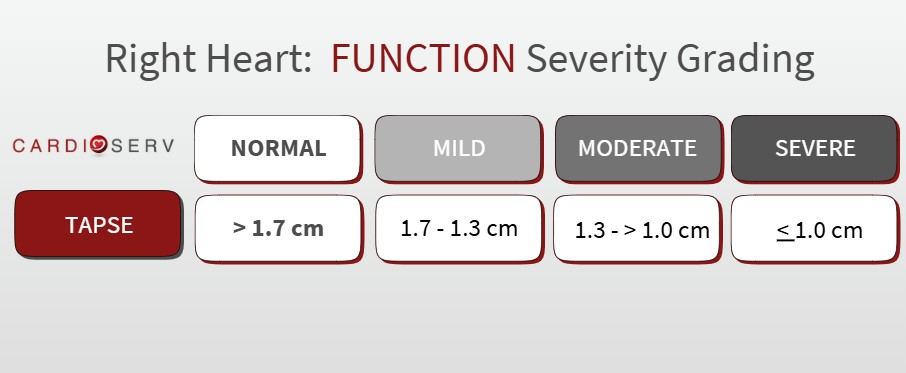
TAPSE Reference Values
The 2025 ASE Right Heart Guidelines maintain the traditional TAPSE cutoff of >1.7 cm for normal function but now introduce graded severity ranges (mild, moderate, severe) for more precise reporting of abnormal findings. The guidelines reaffirm that a TAPSE 1.7 cm or below remains highly suggestive of RV systolic dysfunction.
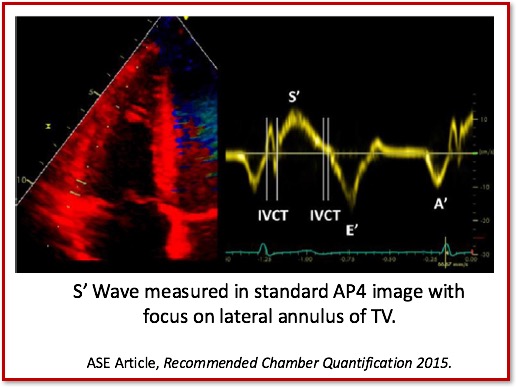
S’ Wave: TDI-Derived Tricuspid Lateral Annular Systolic Velocity
Peak systolic velocity of the tricuspid annulus by Pulsed Wave TDI (cm/sec).
- Good indicator of basal (lateral) free wall function
- Easy to perform & reproduce
- Established prognostic value
- Similar concept to TAPSE
How to perform S’ Wave Measurement
- Place cursor over lateral annulus of tricuspid valve
- Pulse Wave Doppler and TDI
- Decrease gains to avoid measuring ‘noise artifact’
- Identify maximum systolic velocity ABOVE the baseline—‘S’ Wave’
Challenges/Limitations to S’ measurement:
- Angle Dependent
- Not fully representative of global RV function
- Easy to underestimate if Doppler signal is not parallel to annulus
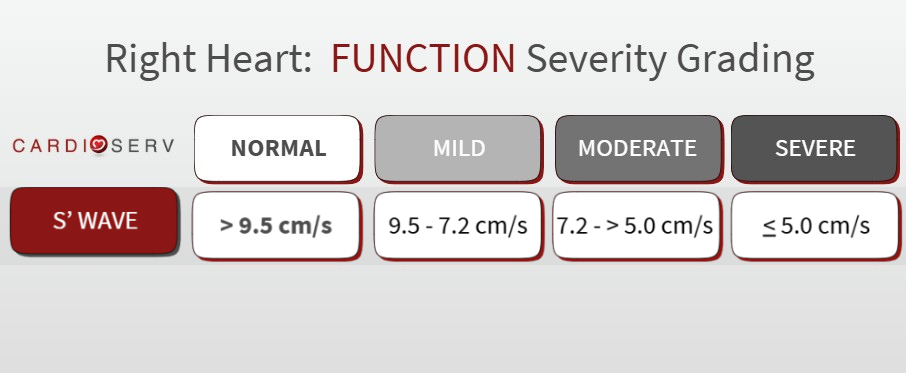
S’ Wave Reference Values
The 2025 ASE Right Heart Guidelines reaffirm S′ wave as a key parameter for assessing RV longitudinal function and refine its reference range slightly. The primary cutoff for normal function >9.5 cm/s. Like TAPSE, S’ wave now also includes graded severity levels of mild, moderate, and severe.
**Important Note
It’s essential to look at TAPSE and S′ together, but they don’t always have to match. An abnormal TAPSE doesn’t automatically mean S′ will be abnormal too, and that’s okay.
The 2025 ASE guidelines emphasize a multiparametric approach to RV systolic function. If TAPSE is reduced, confirm it with other supportive parameters like FAC, 3D RVEF, or RV strain, and always interpret the findings within the clinical context.
In short, no single number tells the full story of RV function. It’s the combination that gives confidence in your interpretation.
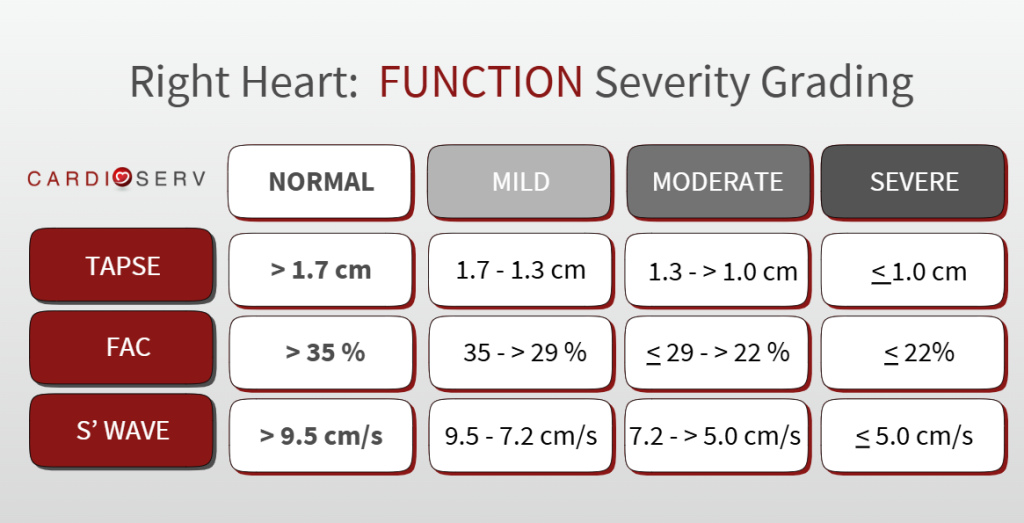
Here is an easy reference chart to refer to in your scanning laboratory:
8 Tips For Measuring TAPSE and S’ Wave on Echo
Implementing TAPSE and S′ in your routine echo exam is straightforward and adds real value to assessing right ventricular systolic function. Here’s how to do it right:
- Use the RV Focused AP4 view
- Utilize chamber focused imaging: we are only interested in the RV & RA!
- Make cursor parallel to motion of annulus!
- Use gain controls to optimize image
- Look for consistent sign for accurate measurement
- Adjust sweep speed to elongate waveforms
- Implement both measurements into your normal scanning routine!
Frequently Asked Questions About TAPSE and Right Ventricular Function
TAPSE (Tricuspid Annular Plane Systolic Excursion) measures how far the lateral tricuspid annulus moves toward the apex of the heart during systole. This reflects the longitudinal shortening of the right ventricle (RV), which is the dominant component of RV systolic function. TAPSE is simple, reproducible, and available in virtually every echo lab, making it one of the most widely used parameters for assessing RV systolic performance.
To measure TAPSE, place the M-mode cursor through the lateral tricuspid annulus in an RV focused apical 4-chamber view. The distance the annulus moves towards the apex from end-diastole to end-systole is recorded, typically in millimeters. It’s a quick and reproducible way to assess right ventricular systolic function.
A normal TAPSE value is considered to be greater than 1.7 cm (>1.7 cm). Values below this threshold are graded by severity into mild, moderate and severe and may suggest right ventricular systolic dysfunction, although it’s important to interpret TAPSE in the context of the entire echocardiogram.
While TAPSE measures the distance the tricuspid annulus moves, the S’ wave measures the velocity of that movement using tissue Doppler imaging. Both are used to assess right ventricular function, but they reflect slightly different aspects of cardiac performance.
TAPSE is primarily a right heart measurement, but left-sided dysfunction can indirectly impact right ventricular performance. When interpreting TAPSE, it’s essential to consider the patient’s overall cardiac function and any contributing conditions.
Go Deeper: Right Heart Quantification in Echo
TAPSE and S′ wave are two of the most commonly used measurements for assessing right ventricular systolic function. Accurate interpretation depends on proper measurement technique, recognizing common pitfalls, and understanding the clinical context.
Our Right Heart Quantification: TAPSE and S′ Wave course walks through practical measurement techniques, interpretation tips, and real echocardiography examples to help you confidently assess RV function.
Learn how to:
• Measure TAPSE correctly in the apical 4-chamber view
• Avoid common S′ wave pitfalls
• Interpret RV systolic function with confidence
Want the Complete RV Assessment Framework?
For a full step-by-step approach to evaluating right ventricular function, explore the All Right Heart Quantification Modules Bundle, which covers the key RV parameters and how they work together in clinical practice.

Andrea Fields MHA, RDCS, Cardiac Clinical Director
References
Mukherjee M, Rudski LG, Addetia K, et al. Guidelines for the echocardiographic assessment of the right heart in adults and special considerations in pulmonary hypertension: Recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr. 2025;38(3):141-186. doi:10.1016/j.echo.2025.01.006
Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39.e14. DOI:10.1016/j.echo.2014.10.003




