Last Updated on October 17, 2025 by Don Gerig, RDCS
Over that past two months, we have discussed various methods for evaluating the right heart. Guided from the updated ASE chamber quantification guidelines, we have been able to elaborate on quantifying methods for:
- Imaging Windows to Optimize Visualization of the Right Heart
- Right Ventricle Size (RVD1)
- Right Atrial Size (RA Volume)
- Right Ventricular Function via:
- TAPSE
- S’ Wave
- FAC
- RIMP
Back in January of this year, we discussed the proper methods for estimating the right atrial pressure (RAP) via echo (which you can find here). This blog covered how to use the collapsibility index to determining the RAP value. If you need a refresher on how to correctly measure the IVC and evaluate collapsibility of the IVC with sniff please review 8 Things to know about estimation of RAP.
This week, we are going to combine the information we have covered on right heart quantification along with the material covered in our RAP blog and review best techniques for acquiring the RVSP (Right Ventricular Systolic Pressure)!
WHAT IS RVSP?
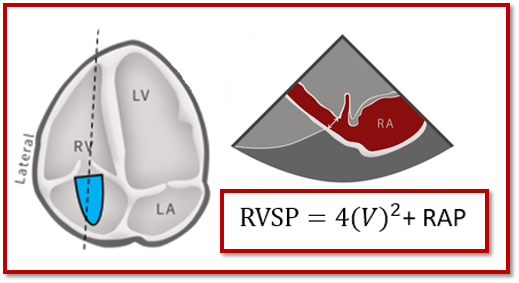
Right ventricle systolic pressure (RVSP) is a measurement commonly found on an echocardiogram that provides us a value estimating the pressure within the pulmonary artery (PA). Pulmonary artery pressures (PAP) are best obtained via cardiac catheterization. Echo allows us to obtain a non-invasive value via RVSP measurement, which tells us the pressure generated by the right side of the heart. RVSP can serve as a guide to help determine the presence of pulmonary hypertension (PHTN) within a patient.
- RV pumps blood to PA, in order for the lungs to receive the blood
- Tricuspid regurgitation (TR) represents pressure difference between RV & RA
- TR causes pressure on right side to elevate
- Higher the TR gradient, the more work on the RV to pump blood to PA
- RVSP can estimate the PA systolic pressure (in absence of RVOT obstruction)
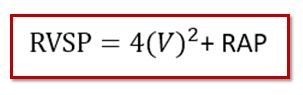
We are able to use the Bernoulli equation to determine the RVSP.
HOW DO WE OBTAIN RVSP?
There are 2 components that contribute to determining the RVSP:
- TR Max Jet Velocity
- Right Atrial Pressure (RAP)
- IVC Size
- IVC Collapsibility
TRICUSPID REGURGITATION VELOCITY
Within our routine scanning protocol, we Doppler the tricuspid valve in order to obtain the peak regurgitant velocity. Since velocity measurements are angle dependent, it is crucial we Doppler the TR gradient in multiple windows. We take the peak velocity obtained and report the value in ‘m/s’.
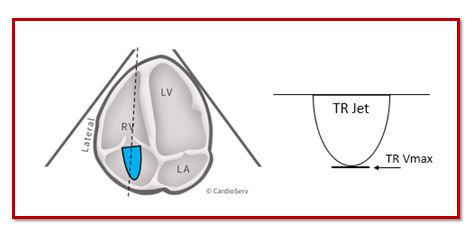
HELPFUL TIPS:
- Doppler cursor parallel to flow
- Doppler Sweep Speed @ 100 mm/s
- Doppler signals should have well-defined border
- Agitated saline can help enhance weak Doppler signals
| ASSESSING RAP VIA COLLAPSIBILITY INDEX | |
| Measure IVC Diameter | Assess IVC Collapsibility with sniff |
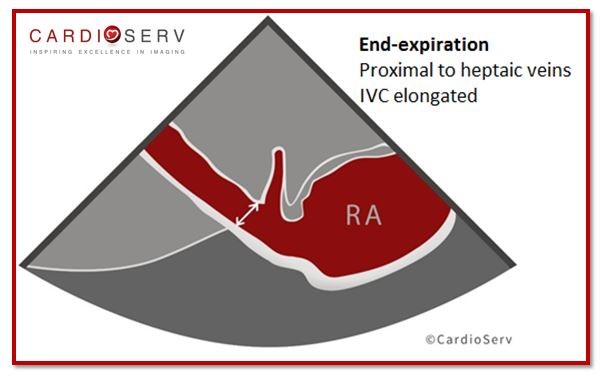 | 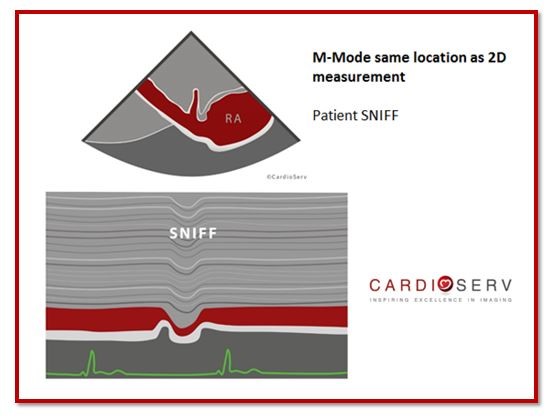 |
| Abnormal > 2.1cm | Abnormal < 50% collapse |
Read the full article on Collapsibility Index: 8 Things to know about estimation of RAP.
RIGHT ATRIAL PRESSURE (RAP):
Once we’ve obtained the IVC diameter and determined collapsibility, we use these variables to estimate our the RAP. ASE released the updated recommended methods for determining the RAP value in the 2015 Chamber Quantification Updates. They suggest moving from a range based RAP to a specific value to help bring simplicity and uniformity to labs!
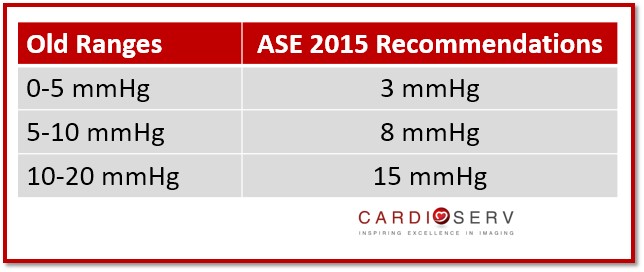
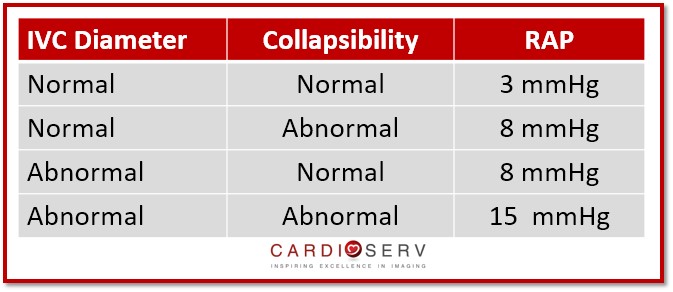
The ASE did a wonderful job with helping us learn how to quickly estimate the RAP value based upon the IVC diameter and collapsibility:
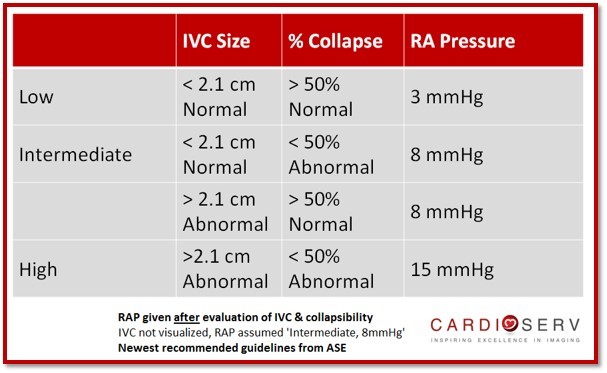
GENERAL RULES TO REMEMBER:
Easiest way to remember the specific RAP value is to understand the normal and high pressure, everything else will fall in the middle category!
- Normal IVC with normal collapsibility = LOW (3 mmHg)
- Abnormal IVC with abnormal collapsibility = HIGH (15 mmHg)
- Any combination of Abnormal & Normal values = INTERMEDIATE (8 mmHg)
- Abnormal IVC, normal collapsibility
- Abnormalcollapsibility, normal IVC
- If IVC cannot be evaluated it is ok to use RAP of 8mmHg
- Do NOT determine RAP until after evaluation of IVC & collapsibility!
RVSP REFERENCE RANGE
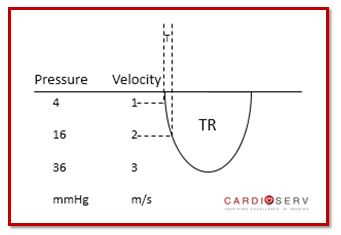
Once we’ve determined the RAP, we are able to then add the TR peak gradient to the RAP to determine the RVSP!
- Cut off range of 35 mmHg, assuming a normal RA pressure of 3
- There is a lot of variability in labs setting their own cut off range
- Due to inconsistency of accurate RAP estimation
- If a lab always uses an RAP of 10 (instead of 3 for normal RAP) this will create a higher cut of range for normal values
- Normal cut of range of 35 mmHg is based on a TR peak velocity of 2.8m/s plus RAP of 3
- TR peak velocity of 2.8 with an inflated value of 10 incorrectly used as the RAP will calculate a RVSP of 40 – This is why many labs use 40 as their cut off
Best practice would be to use the collapsibility index every time when calculating the RAP and be sure to assign the value of 3 in the presence of normal RAP.
SUMMARY
The gold standard for grading pulmonary hypertension (PHTN) is with the Mean Pulmonary Pressure Gradient obtained via cardiac catheterization. With echocardiography the industry standard is to obtain the RVSP and use these values to evaluate for pulmonary hypertension.
According to the 2010 ASE Guidelines for Echocardiographic Assessment of the Right Heart in Adults, they explain a basic concept:
- Simplified Bernouli Equation: RVSP = 4(V)² + RAP
- Systolic Pulmonary Artery Pressure (SPAP) = RVSP (In the absence of RVOT obstruction)
- RVSP ≥ 40 mmHg + Dyspnea = PHTN Present: Further Evaluation Recommended
It is recommended that your laboratory creates a reference value table that is suitable for physicians, staff and patients.
KEY TAKEAWAYS
- RVSP includes the values from TR Peak Velocity & RAP assessed using the Collapsibility Index
- RVSP = SPAP (In the absence of RVOT obstruction)
- Cut off value for normal RVSP is 35 mmHg, assuming a normal RAP of 3
- TR gradients must be obtained in multiple imaging windows
- Ultrasound machine should use the highest TR velocity obtained for accurate RVSP (Make sure your system pulls the ‘Max’ velocity not the ‘average’ into the final report)
- Evaluate the IVC and use the collapsibility index to determine RAP (no more just adding 10!!)
We hope you will take this information and implement this into your routine scanning protocol. With the ASE being the leaders in our industry, it’s vital we continue to learn as they provide educational information to us and improve our scanning skills so that we can give our patients the best care possible.
Go Deeper!
Ready to strengthen your understanding of RVSP, RAP estimation, and right-heart hemodynamics?
Enroll in our Right Heart Quantification & Hemodynamics CME course for a step-by-step review of the 2025 ASE guideline framework. You’ll learn how to integrate Doppler, IVC, and TR data for accurate pressure estimation—and earn CME credit while doing it.


Andrea Fields MHA, RDCS, Cardiac Clinical Director
References
Lang, R. M., MD, Badano, L. P., MD, & Mor-Avi, V., PhD. (2015). Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. JASE, 28(1), 1-53. Retrieved March 1, 2017, from http://asecho.org/wordpress/wp-content/uploads/2015/01/ChamberQuantification2015.pdf
Rudski, L. G., MD, & Lai, W. W., MD. (july 2010). Guidelines for Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography. JASE,23(7), 1-29. Retrieved April 11, 2017, from http://www.onlinejase.com/article/S0894-7317(10)00434-7/pdf




