
Last Updated on April 29, 2026 by Don Gerig, RDCS
Right atrial (RA) size has traditionally been viewed as a supporting measurement. That is no longer the case.
In the 2025 ASE Right Heart Guidelines, RA size has been shown to play a direct role in pulmonary hypertension (PH) screening, risk stratification, and prognosis.
This shift makes accurate measurements of the right atrium more important than ever.
Getting it right requires more than tracing a chamber. It depends on:
- Proper image acquisition
- Correct timing in the cardiac cycle
- Standardized measurement techniques
- Updated reference values and severity grading
This guide walks through how to measure the right atrium correctly using 2025 ASE recommendations and how to apply those measurements in clinical practice.
How to Properly Image the Right Atrium
Measuring the right atrium correctly starts with getting the right view.
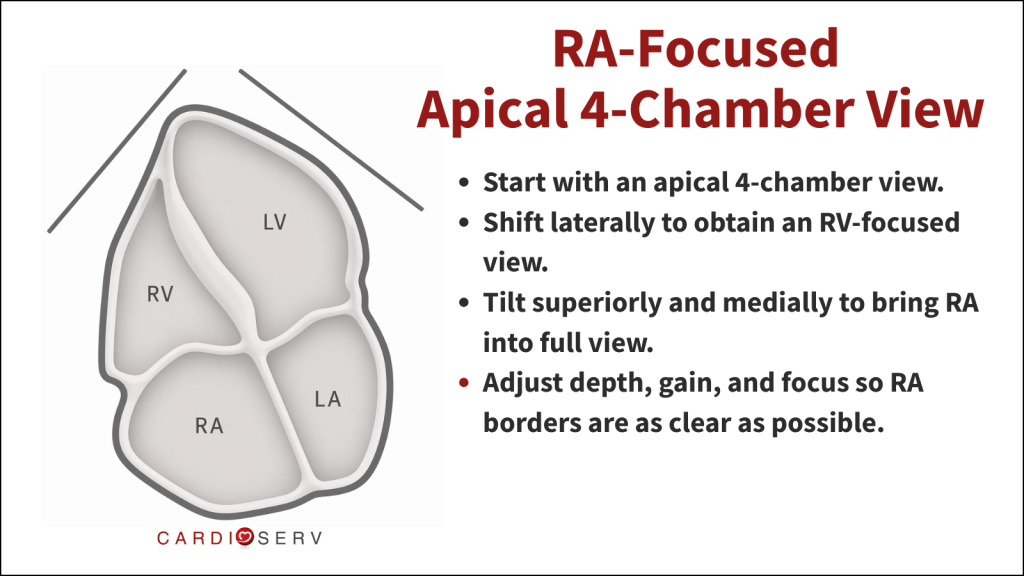
Rather than relying on a standard apical 4-chamber view, the 2025 guidelines recommend using a dedicated RA-focused apical view. This helps you see the full chamber more clearly and reduces the chance of underestimating RA size.
Step-by-step Approach:
- Start with an apical 4-chamber view.
- Shift slightly lateral to obtain an RV-focused view.
- Tilt superiorly and medially to fully visualize the right atrium.
- Adjust depth, gain, and focus so RA borders are as clear as possible.
The goal is to see the entire right atrium without foreshortening.
A foreshortened view can make the chamber look smaller than it really is, which can lead to inaccurate measurements and underreporting of RA enlargement.
RA-Focused Apical View
How To Measure The Right Atrium
The American Society of Echocardiography recommends two methods for assessing right atrial (RA) size:
- RA volume measurement (2D single plane method of discs or the area-length method)
- Linear dimensions (major and minor axes)
RA Volume Measurement
RA volume provides a more complete and representative assessment of atrial size compared to linear measurements. The benefits of RA volume over linear measurements include:
- More representation of the actual RA size
- More robust and accurate values compared to linear measurements
Linear Dimensions (Major and Minor Axis)
RA major and RA minor dimensions are still included as standard measurements and should also be obtained from a dedicated RA-focused apical 4-chamber view. However, they are less representative of true RA size compared with volumetric assessment.
How To Perform Correct RA Volume Measurement
Once you have a good view of the right atrium, the next step is measuring it.
RA volume can be calculated using either the single-plane method of discs (MOD) or the area-length method. That said, the 2025 ASE guidelines clearly favor the method of discs as the preferred approach because it provides more consistent and reliable measurements.
No matter which method you use, the fundamentals stay the same:
- Obtain an RA focused apical 4-chamber view
- Measure at end-systole when the RA is at its largest size
- Exclude tracing IVC, SVC and RA appendage
2D Single Plane Method of Discs
- Trace the right atrium from the level of tricuspid valve annulus
- The software package will connect the two annulus sides with a straight line
- Remember the length MUST be perpendicular to the straight line connecting the two annulus sides. This is important for accurate disc summation calculations.
Area-Length
- Area
- Trace the right atrium from the level of tricuspid valve annulus
- Connect two annulus sides with a straight line across
- Length
- Length is perpendicular to annular plane
Right Atrial Volume Reference Ranges For Echo
Reference values differ depending on the method used.
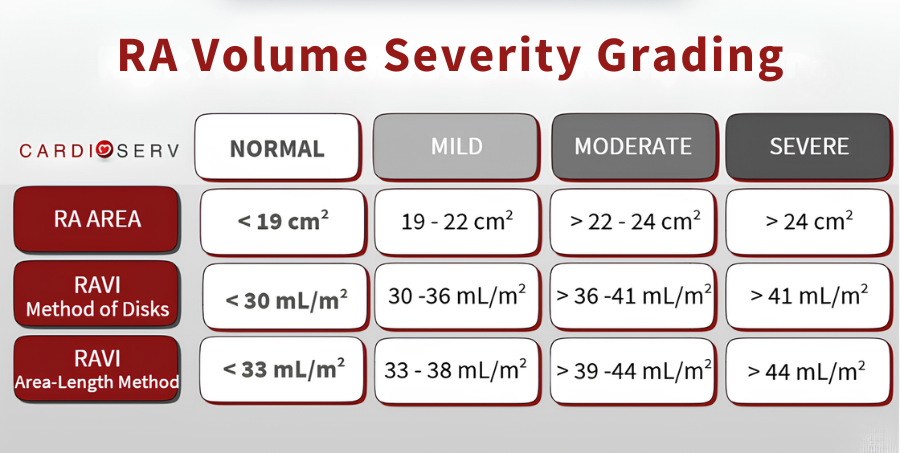
RAV Index (Method of Discs)
- Normal: < 30 mL/m²
- Mild: 30–36 mL/m²
- Moderate: >36–41 mL/m²
- Severe: >41 mL/m²
Area-Length Method
- Normal: < 33 mL/m²
- Mild: 33–38 mL/m²
- Moderate: 39–44 mL/m²
- Severe: >44 mL/m²
RA Area
- Normal: < 19 cm²
- Mild: 19–22 cm²
- Moderate: >22–24 cm²
- Severe: >24 cm²
How to Measure RA Size with Linear Measurements
The right atrium is a three-dimensional structure, which is why volumetric assessment is preferred.
However, in real-world scanning, there are situations where endocardial borders are not well visualized, making accurate volume measurement difficult.
In these cases, 2D linear measurements remain an acceptable alternative.
The two measurements to obtain are the:
- RA Minor Axis (width)
- RA Major Axis (length)
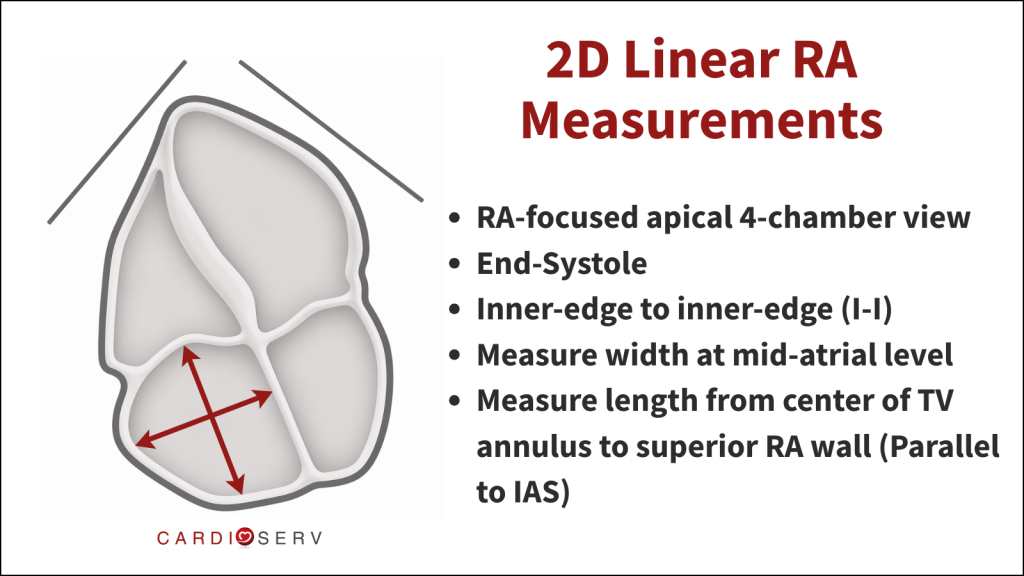
How to perform RA Linear Measurements:
- Use a dedicated RA-focused apical 4-chamber view
- Measure at end-Systole (largest RA size)
RA Minor Axis (width):
- Measure the width from the lateral right atrial wall to the interatrial septum (IAS)
- At mid-atrial level
- Inner-edge to inner-edge (I-I)
RA Major Axis (length):
- Measure the length from center of valve annulus to center of superior RA wall
- Parallel to the intra-atrial septum (IAS)
- Inner-edge to inner-edge (I-I)
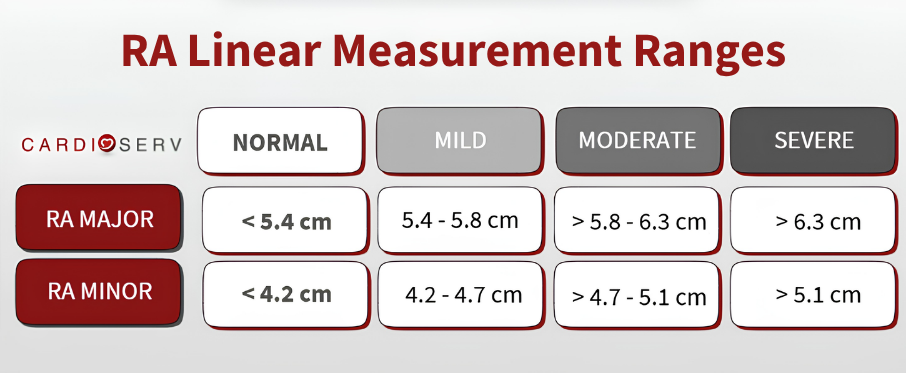
Right Atrial Linear Reference Ranges For Echo
When To Measure The Right Atrium
Getting the timing right is just as important as getting the view right. When measuring the right heart, the RA and RV are not measured at the same point in the cardiac cycle, and this is a common source of error.
Here’s the key distinction to remember:
- Right atrium (RA) is measured at end-systole, when it reaches its maximum volume
- Right ventricle (RV) is measured at end-diastole, when it is at its largest size
It sounds simple, but mixing these up can lead to inaccurate chamber sizing. If the timing is off, the measurement is off.
10 Tips For Correctly Measuring Right Atrial Size on Echo
1. Use RA Volume as Your Primary Measurement
RA volume is the preferred method for assessing right atrial size. Whenever possible, use indexed RA volume (RAVi) instead of linear dimensions.
2. Use the Method of Discs (MOD)
The 2025 guidelines recommend the single-plane method of discs (MOD) for RA volume. This is the most standardized and reliable 2D approach.
3. Always Index RA Volume to BSA
RA volume should be reported as an indexed value (mL/m²). This is essential for accurate interpretation.
4. Use a Dedicated RA-Focused Apical View
Do not rely on a standard apical 4-chamber view. Instead:
- Start with an RV-focused view
- Tilt superiorly and medially to fully visualize the RA
5. Measure at End-Systole
All RA measurements should be taken at end systole (largest RA size). This is one of the most common sources of error.
6. Trace Carefully and Exclude the Wrong Structures
When tracing the RA, exclude the IVC, SVC and RA appendage.
7. Use Inner-Edge to Inner-Edge (I-I)
Maintain consistency with inner-edge to inner-edge measurements. This applies to both area and linear dimensions.
8. If You Can’t See It Clearly, Don’t Measure It
Incomplete border definition equals unreliable data. Do not measure what you cannot see.
9. Only Use Linear Measurements When Needed
RA volume is the preferred method to measure RA size. However, linear measurements are acceptable if volume cannot be measured.
10. Report RA Size with Clinical Context
RA size is no longer just descriptive. It plays a role in pulmonary hypertension assessment, risk stratification and prognosis. RA enlargement should be interpreted and reported alongside RV size and function, TR severity and RAP.
How To Measure The Right Atrium FAQ
RA-focused apical 4 chamber.
End-systole.
RA volume using method of discs.
RA area <19 cm² or RAVi <30 mL/m².
Summary
Right atrial measurement has evolved from a simple chamber assessment to a clinically meaningful parameter tied to real patient outcomes. The 2025 ASE Right Heart Guidelines provide a more structured and clinically meaningful framework of how to properly evaluate the ‘forgotten right heart’.
Here at CardioServ, we want to help provide you with easy tips to correct quantification techniques. Our goal is to help you confidently integrate right heart quantification into your daily scanning workflow.


References
Mukherjee M, et al. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults and Special Considerations in Pulmonary Hypertension: Recommendations from the American Society of Echocardiography Journal of the American Society of Echocardiography, 38, 141-186 DOI: 10.1016/j.echo.2025.01.006




