Last Updated on October 22, 2025 by Don Gerig, RDCS
As diagnostic imaging professionals, we often perform echocardiograms on patients with hypertension to monitor the thickness, strength and wall motion of the heart. Last week we launched our two-part blog on left ventricular hypertrophy (LVH). In part one of Understanding LVH: Concentric, Eccentric and Concentric Remodeling, we explained the pathophysiology behind the various categories of LVH along with the echocardiographic findings. We discussed how LVM and RWT plays a role in identifying the categories of LVH. This week we will answer the question: What is LVM and RWT and how do we obtain these values?
Left Ventricular Mass (LVM) and Relative Wall Thickness (RWT)
- LVM is the acronym for Left Ventricular Mass. LV mass (LVM) is a vital prognostic measurement we obtain with echocardiography to manage hypertension.
- RWT is the acronym for Relative Wall Thickness and is an additional reference value that can help further classify the type of LVH.
How Do We Determine LVM and RWT?
- Both the LVM and RWT are values calculated using a formula.
- Both formulas require accurate measurements of the LV wall thickness and LV chamber.
- There are different formulas that can be used to calculate these values based on how you measured the LV wall thickness and LV chamber size.
- We will teach the Linear ‘Cube’ Method due to:
- Ease of use
- Reproducibility
- Wealth of published data demonstrating prognostic value
LVM: Linear Cube Method Formula
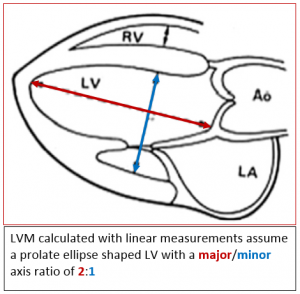
All LVM algorithms are based on the subtraction of the LV cavity from the LV epicardium. The formula used for calculating the LV mass from linear dimensions assumes an ellipse shape with a major/minor axis ratio of 2:1. Needless to say, if you do not have a prolated ellipsed shaped LV this would not be the best formula to use!
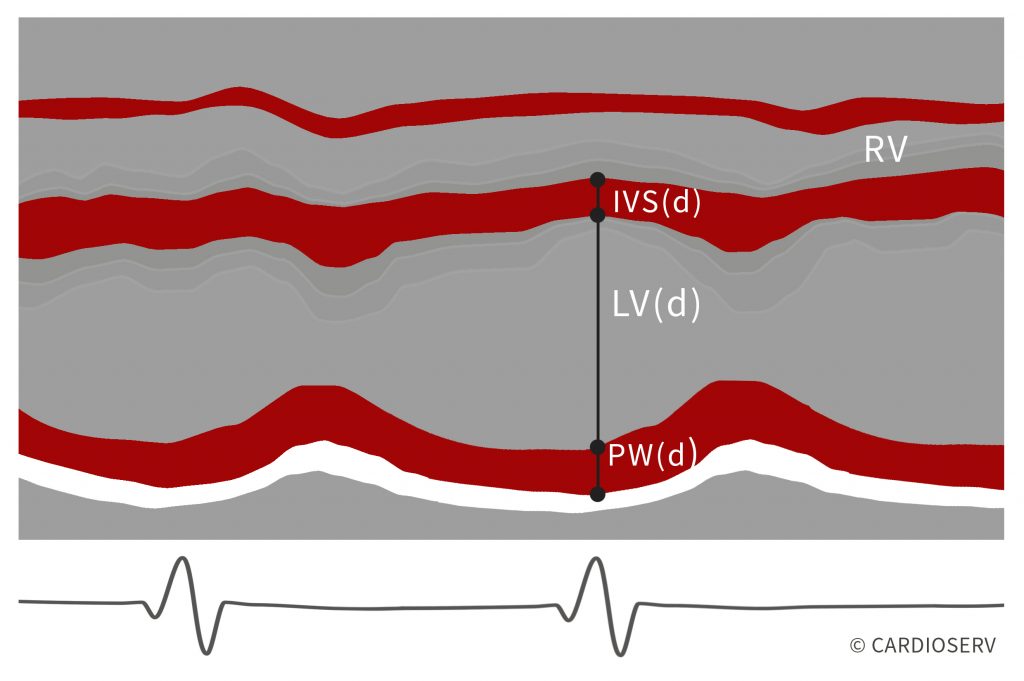
Based upon the assumption of a normally shaped Left Ventricle the Cube Formula uses the following linear measurements:
- IVS(d) – Interventricular septum diastole
- LV(d) – Left ventricle diastole
- PW(d) – Posterior wall diastole
ASE recommends using M-Mode in the parasternal short axis when specifically calculating the LVM but it is ok to use the linear measurements you obtain during your routine study (whether in 2D or M-Mode, PLAX or PSAX). The advantages to M-Mode for LVM include:
- Wealth of published data
- Demonstrated prognostic value
- Simple for screening large populations
Remember that LV Mass (LVM) is a formula that your ultrasound machine will calculate for you, once you enter the measurements needed to complete the formula. You do not need to worry about the actual formula but for all you curious folks here it is:
LVM(g) = 0.8 x 1.04 x [(IVSd + LVd + PWd)3 – LVd3] + 0.6g
Helpful Hints
- The linear Cube method should NOT be used with major distortions of the LV shape (remember the 2:1 ratio rule!)
- Preferred method for Linear Cube LVM calculations is with M-mode is the Parasternal short axis at the basal level of LV
- If using M-mode to obtain your IVS, LV, PW be sure your M-Mode is truly perpendicular to the long axis of the LV
- The formula involves cubing measurements so small mistakes are magnified
- The measurements are dependent on the image quality and the technical quality of the study
I already measure the interventricular septum, LVED and posterior wall but I never see the calculated left ventricular mass!
You need to make sure your ultrasound system is set up to calculate the LVM. Usually this requires going into your configuration menu and selecting which formula you want included in your measurement package. Remember to select the LVM Linear Cube formula. Questions?
- Look at your config. menu
- Call your vendor and ask them how to add this formula – seriously, don’t be shy…call your vendor!
Left Ventricular Mass Reference Guide
To quote ASE: “The main contribution of echocardiography to the management of hypertension is the assessment of left ventricular mass (LVM)”. We need to start reporting on LV Mass on all patients with hypertension. The normal reference range for LVM is gender specific and indexed to BSA.
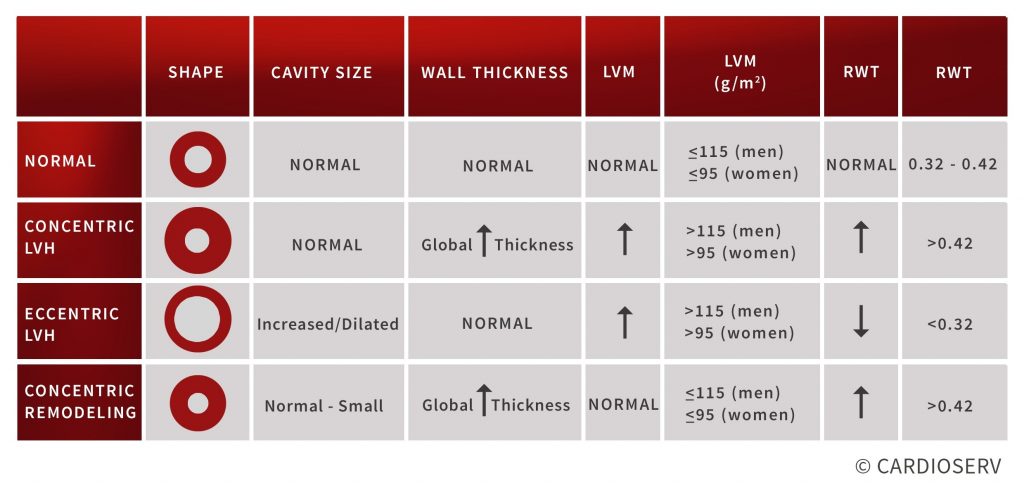
- Concentric LVH = increased LVM
- Eccentric LVH = increased LVM
- Concentric remodeling = normal LVM

Relative Wall Thickness (RWT)
Relative Wall Thickness helps calculate if the ventricular morphology has altered. The RWT reports the relationship between the wall thickness and cavity size. The RWT is calculated by doubling the dimension of the posterior wall and dividing by the LV dimension.
RWT = ( 2 x PWd ) / LVd
Another variable of this equation would be to add the IVS and PW instead of multiplying the PW by two. The reason this method is less preferred is because septal measurements may be confounded by the presence of septal bulge.
RWT = (IVSd + PWd) / LVd
Remember that Relative Wall Thickness (RWT) is also just a formula. Your ultrasound machine will calculate this for you once you enter the measurements needed to complete the formula. Again, you will already have obtained your posterior wall (PWd) and left ventricular dimensions (LVd). You will just need to make sure your ultrasound system is set up to calculate and display the RWT formula.
Relative Wall Thickness Reference Guide
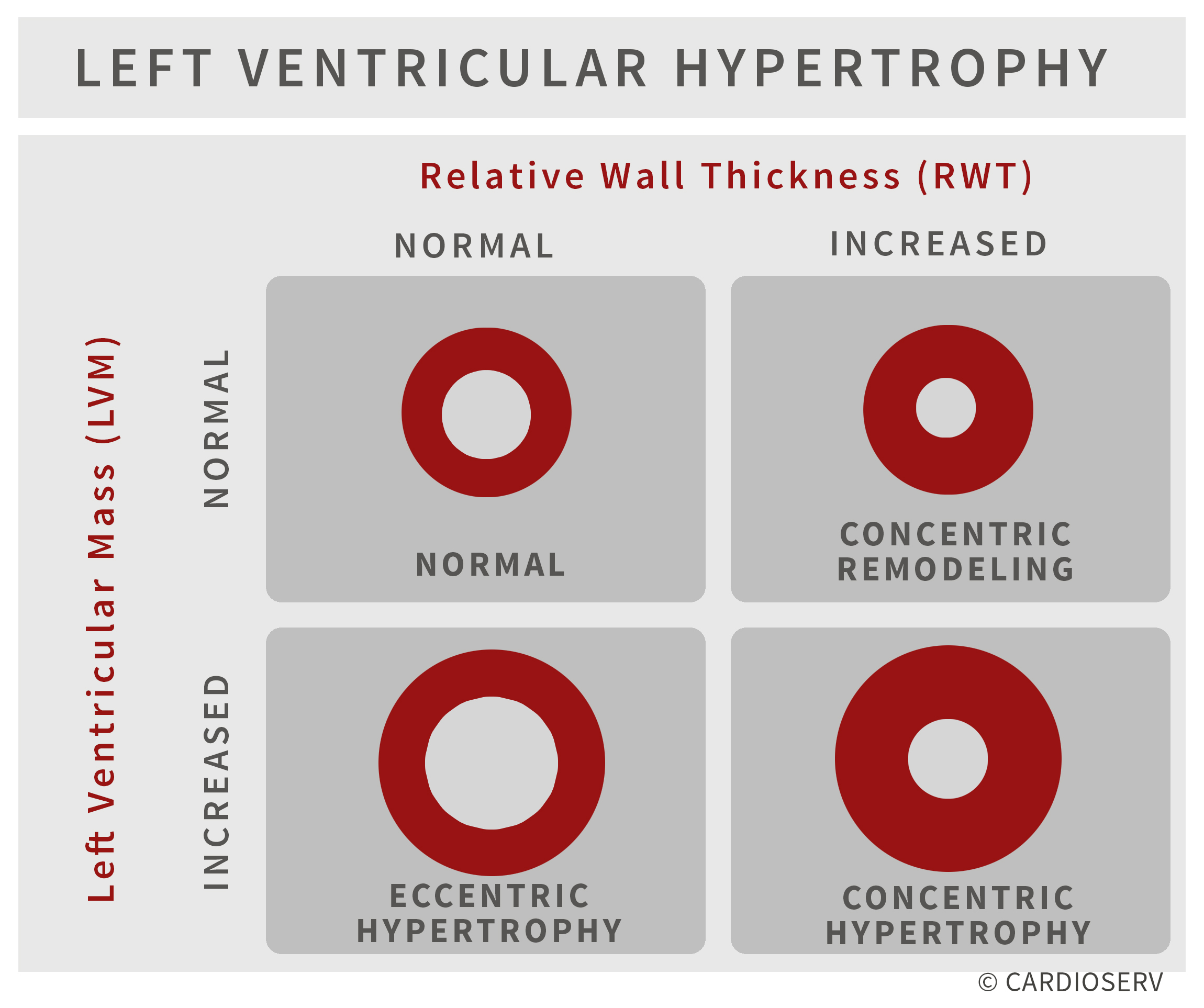
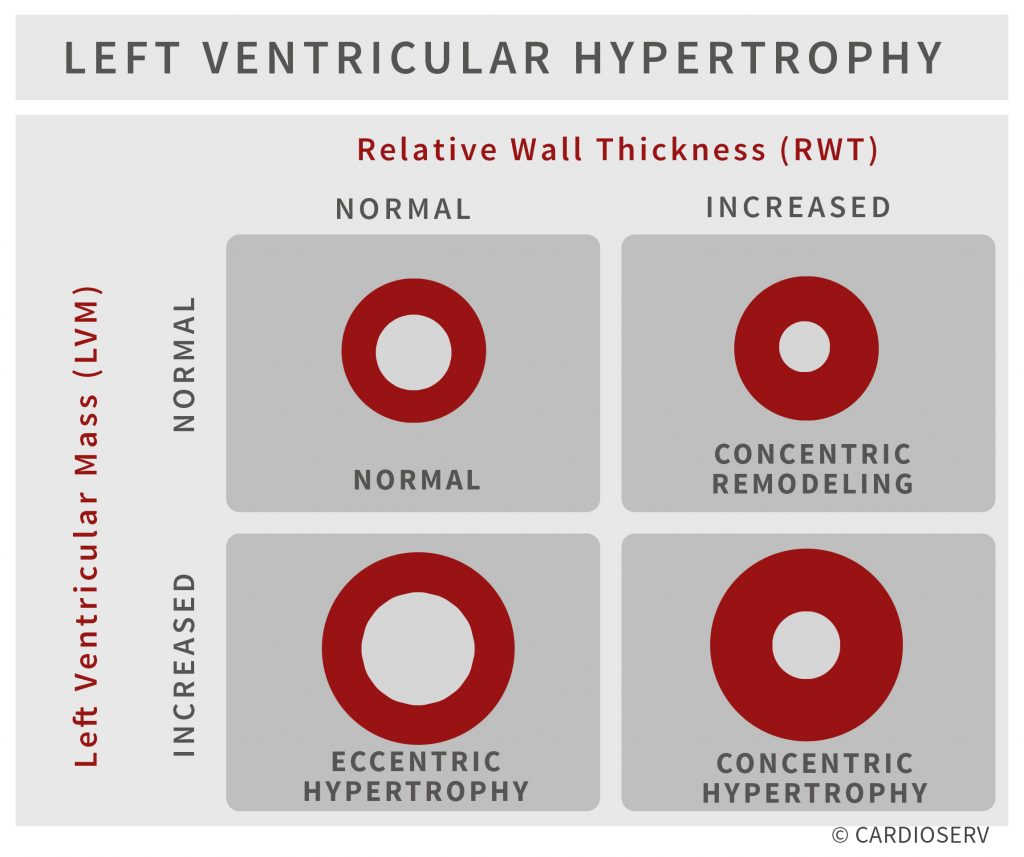
The ASE recommends “Description of LV geometry, using at the minimum the four categories of normal geometry, concentric remodeling, and concentric and eccentric hypertrophy,
should be a standard component of the echocardiography report.” The normal reference range for RWT is 0.32 – 0.42 regardless of gender or BSA.
- Concentric LVH = increased RWT
- Eccentric LVH = decreased RWT
- Concentric remodeling = increased RWT

Summary
- Both LV Mass (LVM) and Relative Wall Thickness (RWT) are calculations that provide you with additional information to better categorize the type of left ventricular hypertrophy.
- Both these calculations require accurate assessment of the LV cavity size and wall thickness
- This article explained the linear method (cube formula) for calculating these values
- You already measure the required elements of these formulas during a routine echo
- Adjusting the settings on your ultrasound machine will allow you to calculate these values
- Contact your ultrasound vendor (or look in the configuration menu) to display these values on your system