Last Updated on November 18, 2025 by Don Gerig, RDCS
Last week we reviewed some common errors found when measuring diastolic function. This week we will review the 5 steps to identify diastolic dysfunction in echo. Since the Intersocietal Accreditation Commission mandates both the assessment and reporting of diastolic function for echo accreditation, we thought it would be a good idea to review these measurements again. We understand that diastology can be complex, but this is a great starting point.
Before we can grade the severity of diastolic dysfunction, we first have to know if diastolic dysfunction is present. We have posted similar articles on diastology. This week we will address how to establish if diastolic dysfunction is present in a patient with a normal ejection fraction and no known cardiac disease.
IDENTIFY DIASTOLIC DYSFUNCTION: STEP 1
LEFT VENTRICLE EJECTION FRACTION
The algorithm we are going to use to determine the presence of diastolic dysfunction is specifically for patients with a normal ejection fraction. Therefore, step 1 requires us to calculate the ejection fraction of our patient using the Bi-Plane Simpson’s method. You will need to measure the LV in both systole and diastole in the 4 chamber and 2 chamber view. For additional tips on how best to perform the Bi-plane Simpson’s method for LV volume and EF in echo, review our past blog.
IDENTIFY DIASTOLIC DYSFUNCTION: STEP 2
Mitral Valve Inflow: E Wave
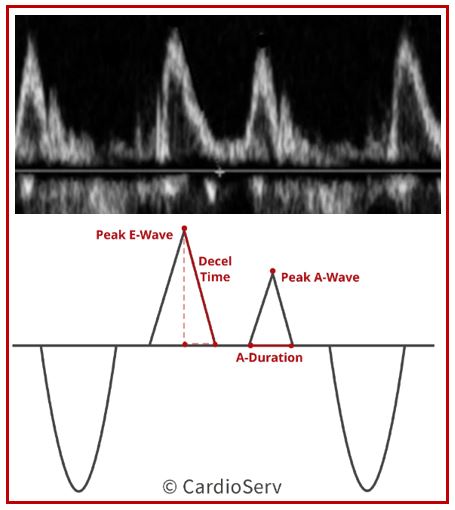
Next, perform an accurate PW of the MV inflow and obtain your peak E Wave velocity. This will be used to determine your average E/e’ measurement. Correct PW technique includes:
- Apical 4 chamber
- Pulsed-wave Doppler
- Sample volume between mitral valve leaflet tips
- Low wall-filter
- E Wave: Early diastole (after T-wave on EKG)
IDENTIFY DIASTOLIC DYSFUNCTION: STEP 3
PW TISSUE DOPPLER IMAGING:
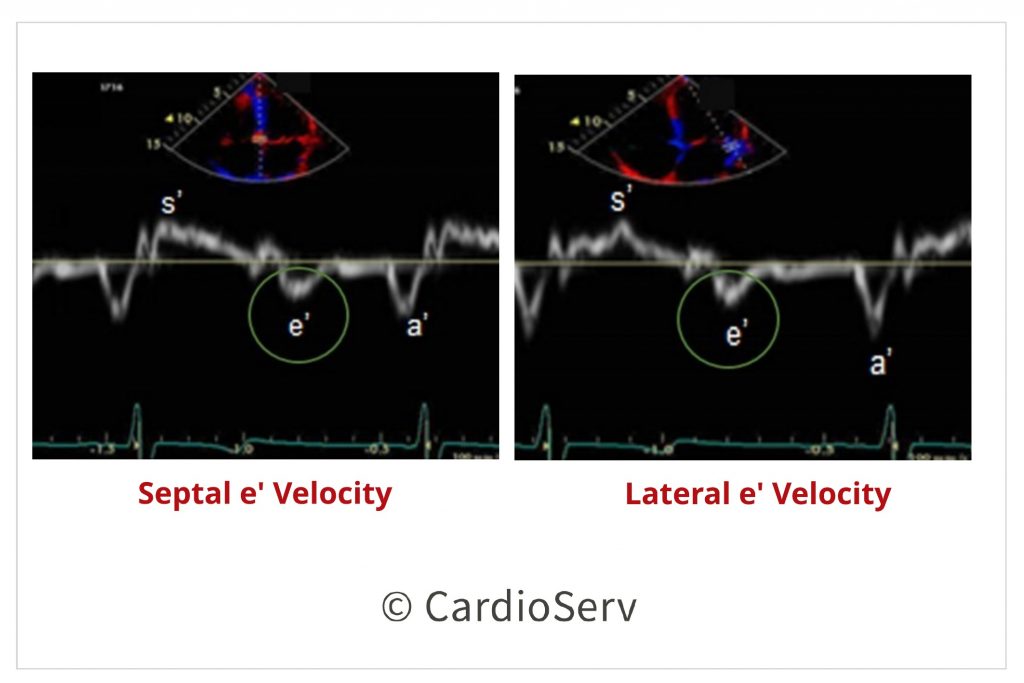
Now onto step 3 – In the 4 chamber view, perform tissue Doppler (TDI) of the mitral valve on both the septal and lateral basal region. For common errors to avoid, check out last weeks blog. This data will provide:
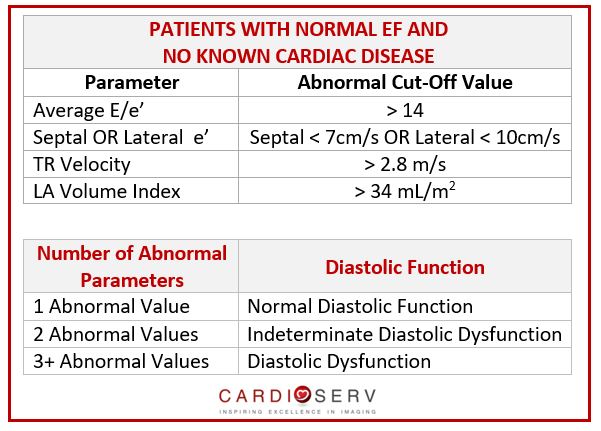
- Average E/e’ (Abnormal cut-off value > 14)*
- Septal e’ velocity (cm/sec) (< 7 cm/s)
- Lateral e’ velocity (cm/sec) (< 10 cm/s)
NOTE: The average E/e’ is calculated using the average value of both the septal and lateral TDI velocities.
IDENTIFY DIASTOLIC DYSFUNCTION: STEP 4
TRICUSPID REGURGITATION
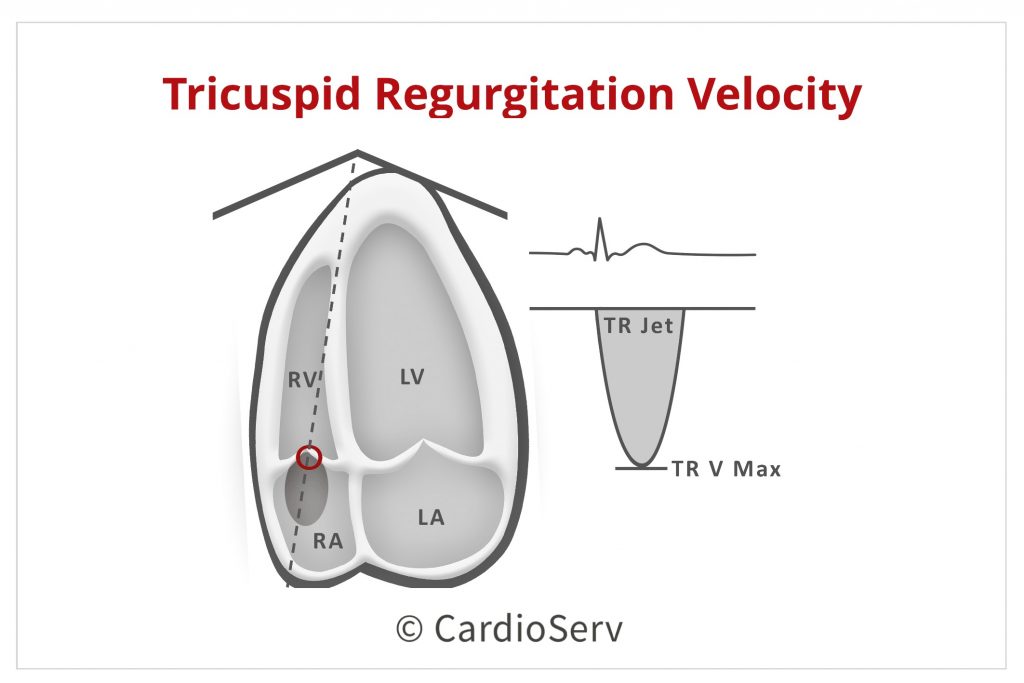
Step 4. It is necessary to know the max tricuspid regurgitation (TR) velocity when determining LV dysfunction. We have a past blog that covers the tricuspid valve and how to calculate the RVSP in echo. In regards to diastology assessment, we are looking at the max TR velocity. The abnormal range used in diastology assessment is a TR velocity > 2.8 m/s.
DIASTOLIC FUNCTION IN ECHO: STEP 5
LEFT ATRIUM SIZE
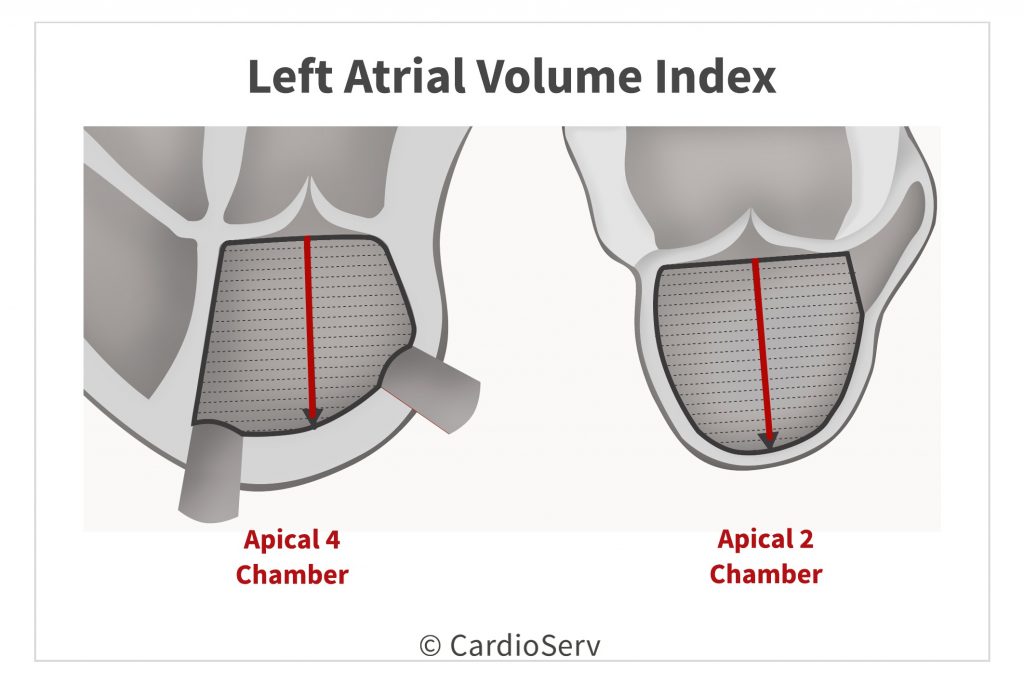
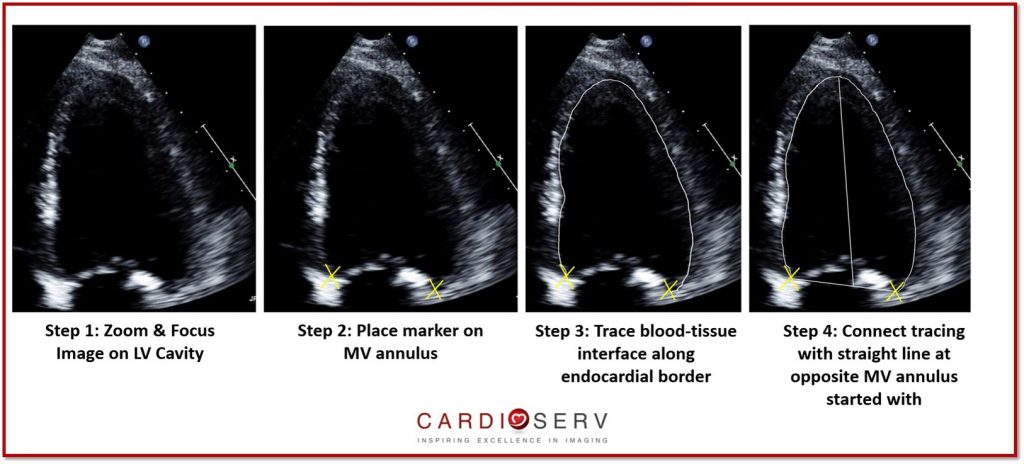
You’ve made it to the last step! The final measurement we must have in order to evaluate for diastolic dysfunction is the left atrial volume index (LAVI). This measurement is indexed to the patients BSA so be sure to enter the patients height and weight into your ultrasound machine in order to calculate the correct LA volume index.
For this measurement, you will trace the LA in end-systole in both the 4 chamber and 2 chamber views. Be careful not to foreshorten your views. For more tips on correct echo left atrial volume measurements you can review past blogs. A cut-off value of > 34 mL/m2 is used as one of the parameters of assessment.
NOW WHAT?
Great…you know how to obtain the necessary echo measures to determine diastolic dysfunction … but now what? How do you apply these measurements to assess diastolic function?
In the case of a patient with a normal ejection fraction and no known heart disease (afib, mod-severe MR, etc.), use the following cut-off values to assess the number of abnormal parameters.
- If you have none, or only one abnormal parameter the patient has NORMAL diastolic function
- If you have three or more abnormal parameters, the patient has diastolic dysfunction
- If you have only two abnormal parameters, the patient has indeterminate diastolic dysfunction
SUMMARY
You now have the basics to help you determine if your patient has diastolic dysfunction. In future weeks, we will discuss how to further handle indeterminate diastolic dysfunction along with how to grade the severity of diastolic dysfunction.
Go Deeper! Master Diastolic Function Assessment
ake your diastology skills to the next level with our CME course — Evaluating Diastolic Function on Echo.
Dive deeper into echo-based evaluation of LV filling pressure, e′/E′ indexing, and comprehensive diastolic dysfunction assessment — all in one interactive, expert-led course. Earn CME credit while expanding your diagnostic confidence.





