Last Updated on January 30, 2024 by Hannes van der Merwe
If you have been following along with Parts 1 and 2 of this blog series, you have already learned how important landmarks are in scanning the abdominal vasculature. We provided a step-by-step method for identifying and imaging the abdominal aorta. This week in Part 3, we will discuss tips and techniques to easily identify with ultrasound the branches of the aorta and other important visceral vessels. If you missed the earlier blogs within this series you can find them here:
- Abdominal Ultrasound for Echocardiographers: Part 1
- Abdominal Ultrasound for Echocardiographers: Aorta and IVC – Part 2
STEP 1: IDENTIFY THE MAIN BRANCHES OF THE AORTA
The superior mesenteric artery (SMA) and celiac axis (CA)
From a longitudinal approach the SMA, is seen rising anteriorly and then turning and coursing distally, maintaining a parallel course to the aorta.
- The SMA is the second branch of the abdominal aorta, and the celiac axis (CA) or trunk, is actually the first.
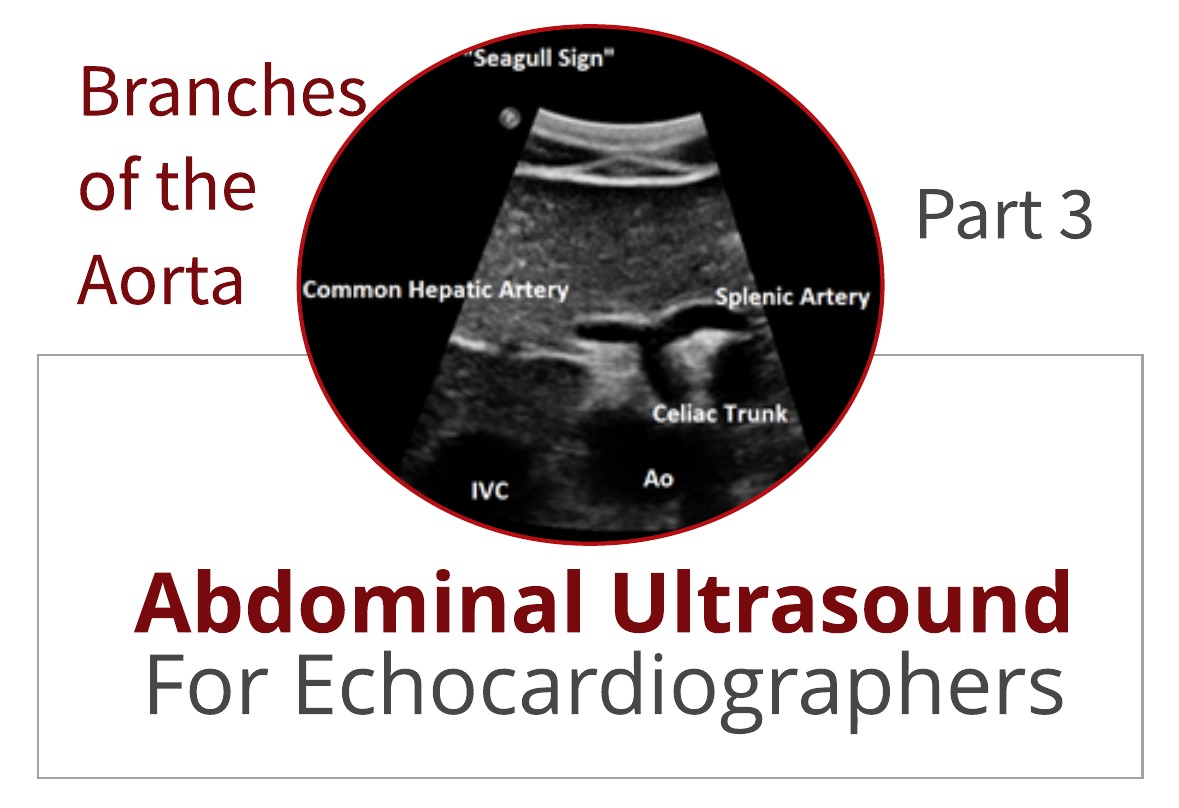
- The CA, rises anteriorly as a very short trunk which quickly divides into 3 branches:
- Common hepatic (easily identifiable)
- Splenic (easily identifiable)
- Left gastric arteries. (rarely seen!)

The celiac axis (CA) or trunk will often parallel the proximal SMA for a very short distance and then give rise to the common hepatic artery (CHA) which courses towards the liver and appears in longitudinal fashion with the transducer in transverse approach.
- At the same level, the splenic artery (SA) courses toward the spleen, also in a longitudinal fashion.
- These 2 branches often create what is known as the “Seagull Sign”. This sign can be very useful in identifying the visceral vessels.


STEP 2: IDENTIFY OTHER VISCERAL VESSELS
Renal Veins
The left renal vein (LRV) is an important abdominal landmark due to its typical location and ease of identification.
- The LRV is a reliable and easily demonstrated vessel and used as a widely accepted abdominal landmark.
- Because it has to course further to reach the IVC, it has a greater length than the right renal vein (RRV).
- The LRV is seen in a longitudinal fashion, anterior to the aorta and posterior to the SMA in a transverse approach as you scan just distal to the SMA.
- The LRV empties into the IVC which will appear in transverse fashion.

Renal Arteries
The right and left renal arteries arise laterally from the aorta just distal to the origin of the SMA and at the level of the LRV.
- They both course posteriorly toward their respective kidneys.
- It is not unusual to see multiple renal arteries!
- The right renal artery (RRA) typically originates at the 10-11 o’clock position and the left renal artery (LRA) close to the 4 o’clock position.
- The renal arteries can be much harder to image than the left renal vein so use the LRV as your landmark! It will help you more easily identify your location.
- Knowing whether the renal arteries are involved in an abdominal aortic aneurysm (AAA) is critical to surgical planning.

SUMMARY
This week we reviewed the best ways to identify the branches of the aorta with 2D ultrasound. We can see how landmarks help us to better identify hard to image vessels. Next week we will discuss the spectral waveform analysis and learn about the hemodynamics of high and low resistance vascular beds.

Yvonne Prince ACS, RDCS, RVT, RDMS, FASE
Connect on LinkedIn!
We would like to thank our guest writer Yvonne Prince. Check out the Educator Spotlight that introduces Yvonne to our Imaging Community and read some of her latest blogs:
- Abdominal Ultrasound for Echocardiographers: Part 1,
- Abdominal Ultrasound for Echocardiographers: Aorta and IVC – Part 2
- Two Ways to Properly Assess TR Jet for Accurate RVSP Calculation
- Tips for Accurate Echo Measurement by Applying Geometric Concepts




