Last Updated on January 30, 2024 by Hannes van der Merwe
How often have you found yourself “in over your head” in the abdomen when trying to image the IVC and abdominal aorta? Is imaging the abdominal aorta part of your echo protocol? It is not uncommon for a patient to receive an abdominal ultrasound because the echo findings mentioned the presence of gallstones, abdominal aortic aneurysm (AAA), or some other abnormality. Subsequently, the abdominal ultrasound reveals none of the suspected abnormalities! So, what happened? Did the abnormalities disappear or were there operator errors? This week we will review some basic tips for echocardiographers scanning the abdomen and review:
- Artifacts
- Image Orientation
- Patient Positioning
Next week I will share with you key anatomical landmarks that once you recognize…will make your scanning life a lot easier!
ARTIFACTS AND OTHER CULPRITS
Frequently, the reason for the suspected abnormality was some type of ultrasound artifact. In the case of gallstones, usually a pocket of bowel gas in the right upper quadrant (RUQ) caused shadowing behind a brightly echogenic leading edge which can mimic a contracted gallbladder filled with stones. Movement of stones within the gallbladder is one of the most important diagnostic parameters. This requires different patient positions, sometimes even having the patient stand. This is beyond the scope of the cardiac sonographer.
GALLSTONES V. ARTIFACT
For the curious cardiac sonographer who would like to better prove or disprove gallstones let’s explore how movement of the stones is used to rule out gallstones versus artifact. Two tips to help you differentiate include (1) looking at the movement of gallstones and (2) identifying peristalsis.
Movement of Gallstones
Movement of gallstones within the GB is one of the most important parameters to PROVE that gallstones are present.
- To accomplish this, the patient must be examined in at least two different body positions – for example, supine and right lateral decubitus.
- Frequently, I would scan the GB as the patient turned. In some cases I have even had to have the patient stand while I scanned the GB.
- Other defects within the GB, such as polyps or septations, will NOT show gravity dependence or movement.
- In the case of a contracted GB with stones, movement of the stones may not occur with changes in positions due to the fact that there is simply not any “real estate” in which they can move.
Peristalsis of bowel gas versus gallstones
- Bowel gas can sometimes create echogenic spots with shadowing that mimic gallstones.
- This type of shadowing changes with peristalsis so it is important to just wait a moment to see if the appearance changes.
- The movement of peristalsis is wave-like and exhibits a continually changing pattern therefore it is easy to discern from the movement of gallstones.
- Stones are denser and heavier than the bile in the GB. The gallstones move within the GB with changes in body position but once a new position is established their movement ceases, whereas peristalsis continues no matter which position is assumed.



Calcification of the gallbladder itself can occur making it difficult to see beyond the shadowing cast by the calcified walls. Heavy calcification of the abdominal aorta can lead to misdiagnosis as well. I have even seen instances where the lumbar spine is wrongly identified as the abdominal aorta. In some of these cases, aneurysms were even reported!
Sometimes a severely fatty liver can make it impossible for our sound beam to penetrate far enough to image the IVC or aorta, depending on your scanning approach. In thin patients, one culprit can be an elongated GB which is more superficial than normal and is mistakenly identified as the aorta or perhaps the IVC.
IMAGE ORIENTATION
Ok, so you are a cardiac sonographer getting ready to perform a quick abdominal scan using your echo probe. Most ultrasound machines have a preset for abdominal settings. Take a look at your machine and see. The abdominal settings are preset to optimize your image.
The first thing to be aware of as an echocardiographer scanning the abdomen is the screen orientation.
- With a typical abdominal preset, the reference icon is on the left of the image and the reference marker on the probe is directed towards the PATIENT’S right side.
- With echo the reference icon is on the right!
- If your machine has an abdominal preset it will automatically switch the screen reference icon. If you do not have an abdominal preset, you can switch the reference icon manually.
- Scanning the abdomen with the icon on the left will allow the structures to be imaged in a conventional manner.
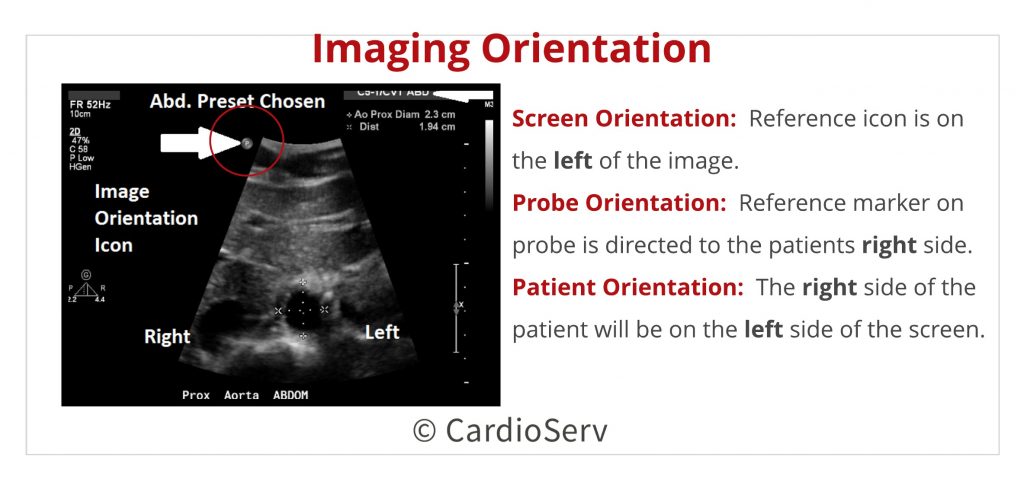
The right side of the patient will be on the left side of the screen as if you are looking face-to-face at the patient. With the patient supine and their knees bent or propped on pillows, scan in a transverse, or “short axis” plane for you echocardiographers, beginning just under the xiphoid process.
PATIENT POSITIONING
So now you have your equipment set up, its time to position your patient. If you are performing a quick scan after an echo, your patient is probably already lying supine due to most echo protocols ending with subcostal views. Here are four hacks for image optimization when performing an abdominal ultrasound scan.
4 Patient Positioning Hacks!
- Having the patient’s knees bent or propped allows for easier access to the abdominal structures by relaxing the abdominal muscles.
- Breath-holding techniques are often needed to bring the abdominal organs into view from this approach.
- Deep breathing displaces the abdominal organs distally as the lungs fill and the diaphragm moves caudally.
- Taking advantage of your patient’s ability to change positions can make the seemingly impossible become possible!
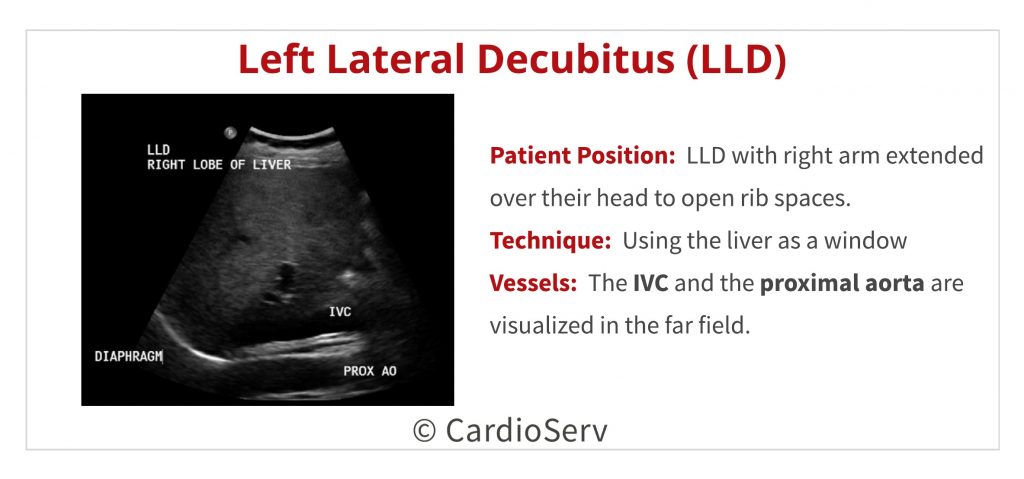
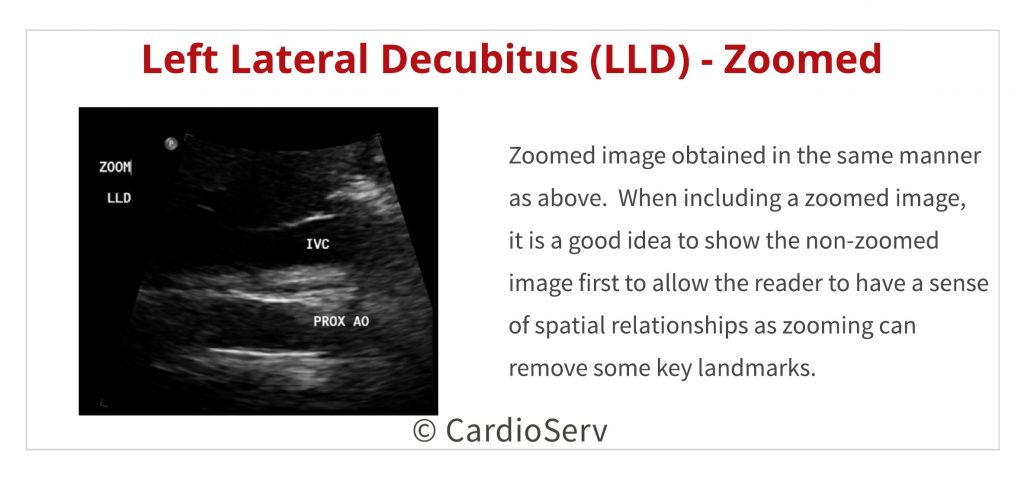
- If you are struggling with imaging the IVC and proximal aorta with your patient supine, roll them onto their left side (left lateral decubitus – LLD) and use the liver as your window.
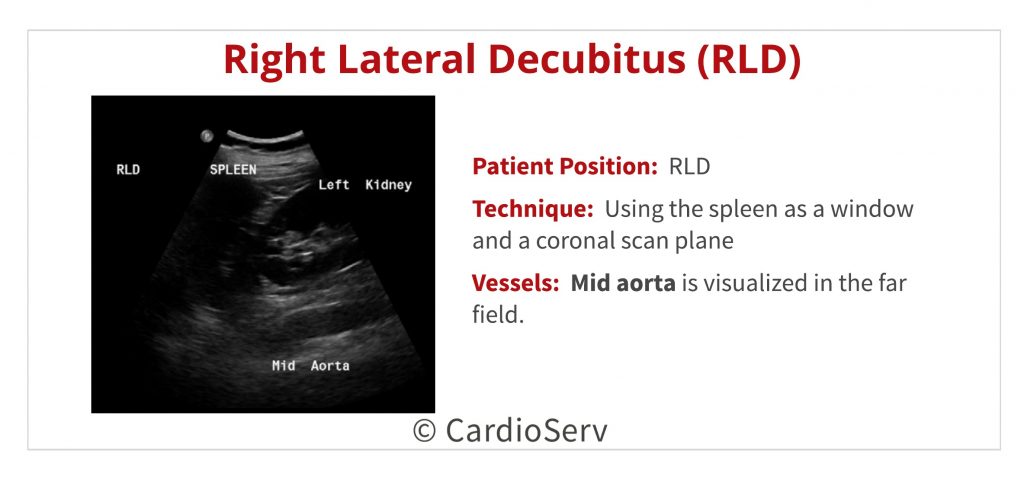
- Having the patient turn into a right lateral decubitus (RLD) position can also be used to image the abdominal aorta by scanning through the spleen, similar to the method described above for using the liver as a window.
- Oblique body angles may prove valuable especially when dealing with patients with large, pendulous abdomens, as turning the patient away or towards you will allow the lipomatous abdomen to move out of the way, thus decreasing the depth needed to reach the aorta, etc., and facilitates the use of less probe pressure.
NEXT WEEK
Having learned to scan in the days before the introduction of color Doppler (yes, I was scanning before the dawn of time!), I learned to rely on my recognition of abdominal landmarks to correctly identify visceral vessels and other structures. When I began to learn echo, this knowledge proved to be priceless. So, just how much abdominal anatomy do you really need to know? Next week, I am going to share with you some of the key abdominal landmarks you need to recognize to make your scanning life easier! Next week we will walk step by step through an abdominal scan using key landmarks to guide you!

Yvonne Prince ACS, RDCS, RVT, RDMS, FASE
Connect on LinkedIn!
We would like to thank our guest writer Yvonne Prince, ACS, RDCS, RVT, RDMS. Check out the Educator Spotlight that introduces Yvonne to our Imaging Community and read some of her latest blogs:
Two Ways to Properly Assess TR Jet for Accurate RVSP Calculation
Tips for Accurate Echo Measurement by Applying Geometric Concepts




