Last Updated on January 30, 2024 by Hannes van der Merwe
Let’s talk about some basic hemodynamics that take affect when evaluating mitral regurgitation (MR). We previously broke down the step by step process the heart encounters when dealing with acute & chronic MR. If you’ve missed or need refreshed on our previous blogs, you can find them here:
- Mitral Valve Anatomy: Name 5 Components!
- Finally… Mitral Valve Orientation Explained!
- Smart Strategies for Determining MR Mechanisms
- Ultimate Guide to Acute vs. Chronic MR
- Essential Steps to Evaluating MR Etiologies
- Secondary MR: Evaluating Mitral Valve Tethering
This week, we are going to touch on a few key items to pay attention to when we are trying to determine the severity of MR.
- Temporal Variation
- Blood Pressure
TEMPORAL VARIATION
It is important to take in consideration the duration & timing of the MR within the cardiac cycle. We need to evaluate this in order to know which quantitative method will provide the most accuracy when determining the severity of MR. We will go further into quantitative methods in our upcoming blogs.
Until then, we need the basic understanding of: At what point during ventricular systole will the regurgitant orifice be at its max? This depends on the mechanism and etiology type of the regurgitant valve.
Let’s take a look at an EKG:
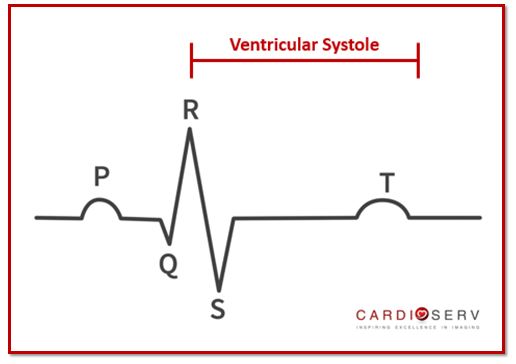
- Ventricular systole occurs from the QRS complex to end of T wave
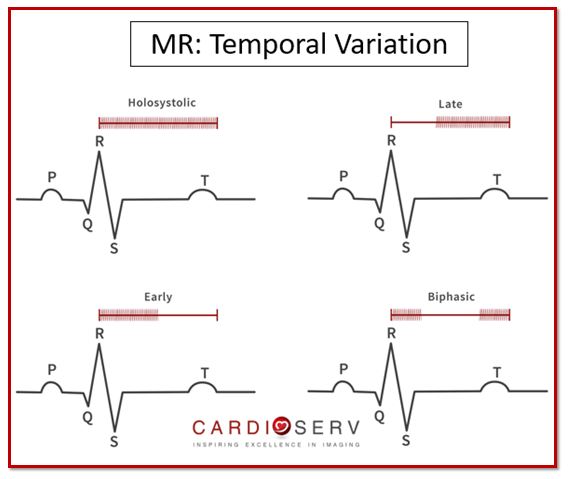
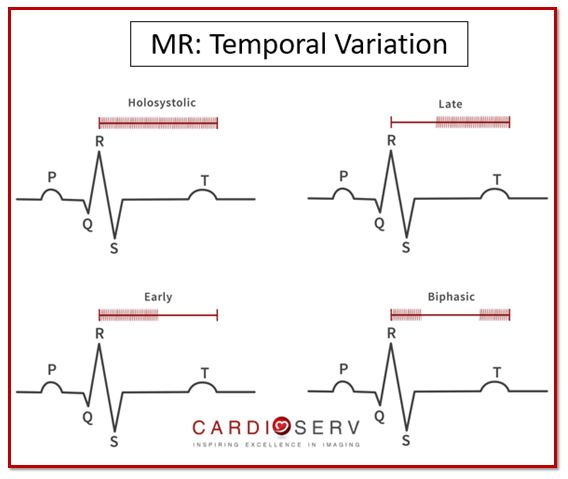
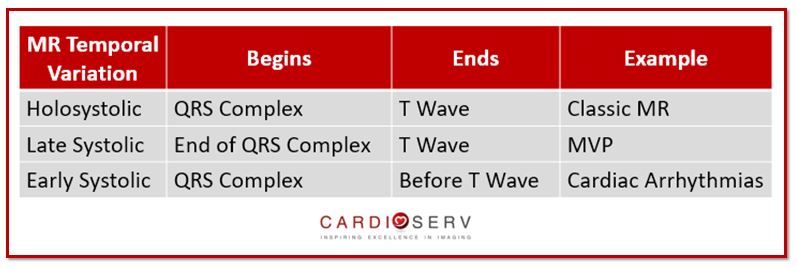
The ASE explains 4 different categories of ‘timing’ when MR can occur:
- Holosystolic: begins at QRS complex & ends at T wave = Classical MR
- Late Systolic: begins towards end of QRS complex & ends at T wave = Mitral Valve Prolapse
- Early Systolic: begins at QRS complex & ends before T wave = Cardiac Arrhythmias
- Biphasic Pattern: initial peak of regurgitation at early systole, then will decline at mid-systole and increase again at late-systole = Secondary MR
We will explain further how the different duration & timing affects the quantitative evaluation in our future blogs.
BLOOD PRESSURE
Blood pressure plays a vital role when evaluating the severity of MR. Before we even begin to scan our patient, we should take an initial blood pressure. It is important to document the pressure at time of study and not use an older pressure in the patients chart.
How does the blood pressure (BP) play such an important role in MR? Blood pressure can dramatically alter the loading conditions and contractility of the heart during the cardiac cycle. This is a perfect example of why we CANNOT BASE MR SEVERITY OFF OF COLOR DOPPLER ONLY!!
Going back to the days of physics: recall that color Doppler involves mass, energy & momentum.
We tend to forget the importance of momentum when utilizing color Doppler on our exams. The ASE explains how the majority of the color jet size is dependent upon momentum! Momentum involves the flow rate, orifice area, velocity & driving pressures (mmHg) within the regurgitant jet. The conservation of momentum explains the amount of momentum within a regurgitant valve will stay constant throughout length of the jet.
How does driving pressures relate to momentum & the appearance of color Doppler jet?
- Decrease Driving Pressures (Hypotension) = Underestimation of MR severity
- Increase Driving Pressures (Hypertension) = Overestimation of MR severity
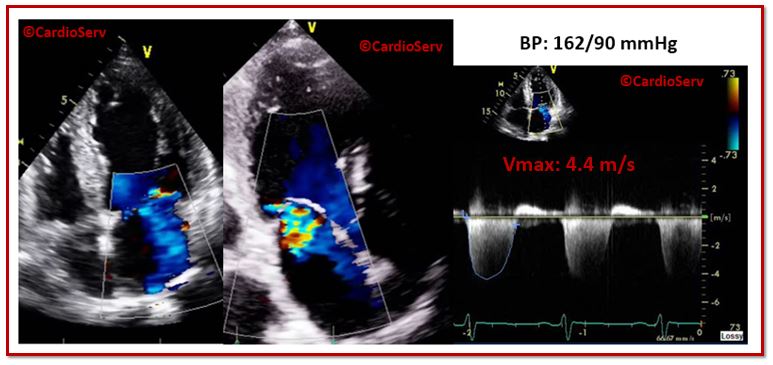
LET’S LOOK AT AN EXAMPLE:
This is the same patient scanned twice between a 4 day window. During the patients first echo, they presented with a BP of 162/90 mmHg. When evaluating ONLY the color Doppler & CW Doppler images, you could assume the severity would most likely be moderate MR.
Four days later the patient had a repeat echo to evaluate the severity of MR with the BP in a more controlled range. The patient arrived with their BP at 110/60 mmHg. Notice the difference when evaluating ONLY the color Doppler & CW Doppler images, this patient clearly has only mild MR.
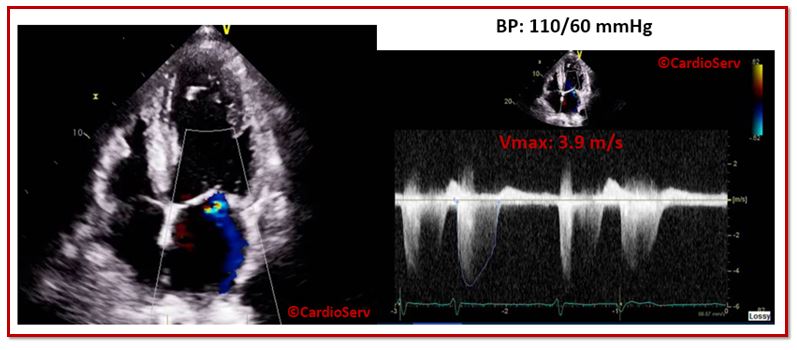
This example explains the importance of why color Doppler cannot be used as the main tool for determining regurgitation severity. Color Doppler and continuous wave Doppler are only qualitative methods for evaluation of MR. We will get further into how to assess this in our upcoming blogs!
SUMMARY
Hemodynamics play a vital role when assessing the severity of mitral regurgitation. As clinicians, we need to remember to evaluate the following information:
- Duration & Timing of Regurgitant Jet
- Blood Pressure at Time of Study
It’s crucial that we do not rely on the color Doppler jet size as the only qualitative method for diagnosing severity of MR. There are too many factors that alter the size, shape and intensity of the signal. That is why we must document the patients blood pressure at time of study. If they are in a hypertensive state, it is important to document that for the physician in order to avoid overestimation of severity. It is best practice to perform a quantitative study when the patients hemodynamic state is within the normal range. As our field grows and advances with new techniques and technology, we must grow and advance with it! This means we must begin to utilize quantitative methods for determining severity, as we advance within our field!

Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Zoghbi, W. A., MD, FASE, & Adams, D., RCS, RDCS, FASE. (2017). Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation. JASE, 30, 4th ser., 1-69. Retrieved June 12, 2017.




