Last Updated on January 30, 2024 by Hannes van der Merwe
HEART FAILURE (HF) – A REASON TO CARE ABOUT RIGHT HEART SIZE AND FUNCTION.
We have been teaching on correct techniques for right heart assessment (including TAPSE and RVSP) for a while now and we still seem to face a little resistance sometimes in regards to the clinical significance of right heart assessment. In order for us to learn and retain information we often have to understand the relevance and make a connection between what we are learning and how it relates to things we know.
How many patients do we see/scan with heart failure? Lots! Often, we are thinking about their left heart function. Did you know that in patients with heart failure (HF) there is a two- to threefold increase in risk of cardiac death with the development of right ventricular dilation and failure? This is irrespective of the severity of LV dysfunction! RV dilation and RV failure are signs of accelerated HF disease progression. This is one of many reasons why assessing the dimensions and function of the right heart is important. Echocardiography is a simple way to obtain reliable markers of RV size and systolic function.
TAPSE AND RVSP RELATIONSHIP AND RATIO.
In earlier blogs we have outlined how to correctly assess the size of the right ventricle and right atrium. Last week we discussed using TAPSE as a method for evaluating RV systolic function because it is easily obtainable, reproducible, and highly predictive of poor outcome in a wide spectrum of HF settings. We have also reviewed how to estimate the RAP via echocardiography to calculate a more accurate RVSP.
Interestingly, these two common assessments (TAPSE and RVSP) are often looked at as individual values. There is a great paper written by M. Guazzi et al that discusses the relationship between these two values and takes into consideration the basic concept that the RV is highly sensitive to the imposed pressure load. The paper reviews the relationship between TAPSE (length) and PASP (developed pressure) and proposed “combining these variables under a ratio may better disclose prognosis compared with either variable in isolation”. I would like to review this study and encourage us to consider a combined assessment of TAPSE and RVSP, which will help us with our clinical decision-making process, and prognosis assessment in daily clinical practice.
Patients were tracked for cardiac mortality resulting from failure of the cardiac system. The study assessed:
- Right heart function via TAPSE (TAPSE blog on correct techniques)
- PASP via RVSP with RAP estimated using the collapsibility index (RAP blog on correct techniques)
- Subjects had no significant RV outflow tract or pulmonic valve obstruction
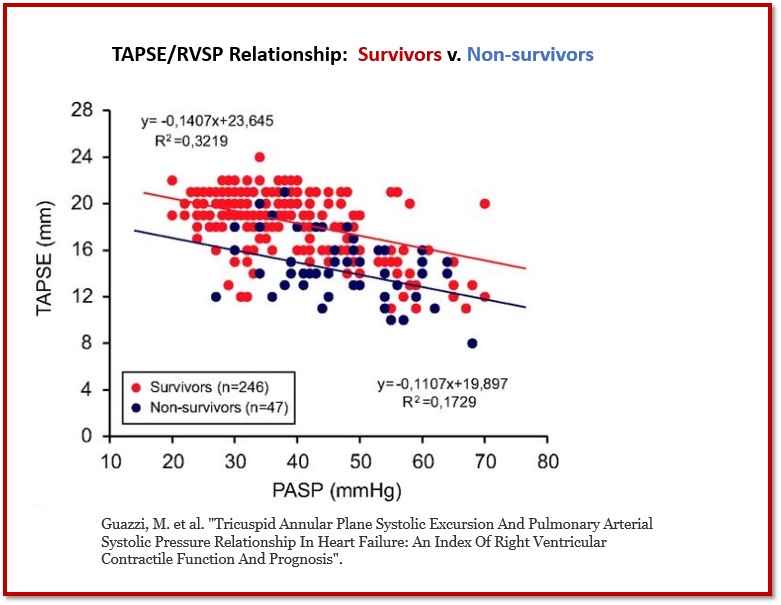
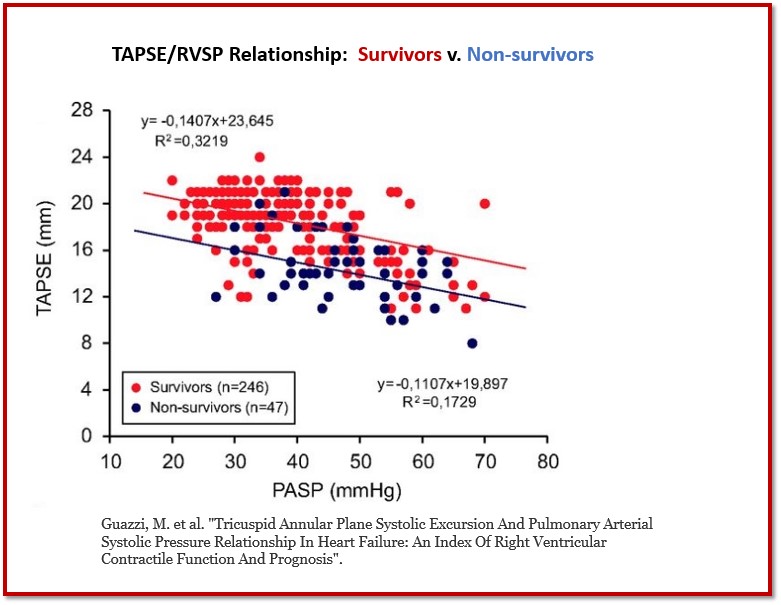
Survivor v. Non-survivor
The following graph demonstrates the TAPSE and RVSP relationship between survivors and non-survivors. The results show a similar downshift of the regression line for non-survivors vs. survivors but of interesting note was that non-survivors had a more unfavorable relationship between having a lower TAPSE with higher PASP values.
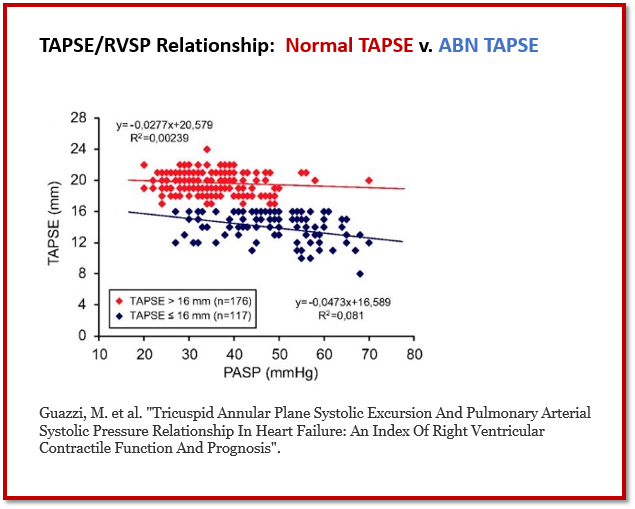
Normal TAPSE V. Abnormal TAPSE
When we look at the results of the TAPSE and RVSP relationship between patients with abnormal TAPSE versus normal TAPSE we see a worsening of the downward shift of regression with abnormal TAPSE values. There was no correlation found between TAPSE and LV ejection fraction.
CONCLUSION OF THE STUDY
The study provided some new insights into RV function evaluation in HF. The relationship of TAPSE and RVSP when viewed as an index instead of individual variables provides a more comprehensive analysis of the right ventricle contractile properties. These findings have both pathophysiological and clinical implications. (Guazzi)
- Echo-derived variables related to RV systolic function are of basic clinical relevance in HF
- The relationship of longitudinal RV fiber shortening (TAPSE) to developed pressure (RVSP) may be viewed as a useful clinical index of the length/force relationship
- The TAPSE/RVSP ratio of the variables potentially possesses a more discerning ability to detect disease severity than each of the two variables separately.
- This approach seems to be worthy of consideration for HF patients presenting with either reduced or preserved LV systolic function
Overall, the information attained seems to be valuable in the daily practice when assessing the right heart in HF syndrome by echocardiography.
HOW THIS AFFECTS OUR DAILY ECHO PRACTICE
We often teach on the correct techniques for obtaining individual measurements and calculations. Often we get locked and loaded on that one variable and forget how all measurements and quantification relates to each other throughout the “story-telling” of an echocardiogram. Our goal is to educate not just on individual techniques but to help clinicians think about the whole heart and how values and variables relate to one another.
WANT A CME FOR READING THIS BLOG? CLICK BELOW TO ACCESS CARDIOSERV’S ONLINE CME PLATFORM OFFERING CAT. 1 AMA CMES!


Judith Buckland, MBA, RDCS, FASE, President
References:
Guazzi, M. et al. “Tricuspid Annular Plane Systolic Excursion And Pulmonary Arterial Systolic Pressure Relationship In Heart Failure: An Index Of Right Ventricular Contractile Function And Prognosis”.
Damy T, et al. “Comparison of four right ventricular systolic echocardiographic parameters to predict adverse outcomes in chronic heart failure.” Eur J Heart Fail 11: 818–824, 2009
de Groote P et al. “Right ventricular systolic function for risk stratification in patients with stable left ventricular systolic dysfunction: comparison of radionuclide angiography to echo Doppler parameters. Eur Heart J 33: 2672–2679,2012.




