Last Updated on February 24, 2026 by Don Gerig, RDCS
Mitral valve anatomy can seem straightforward at first, then suddenly complicated the moment you need to identify a specific scallop or commissure on echo. That is where a clear, structured understanding makes all the difference.
At CardioServ, we want to help break it down into a more enjoyable and practical learning process. Our goal is to help you confidently incorporate this knowledge into your daily scanning practice. In order to identify mitral valve pathology accurately, we must first be comfortable with the basic anatomy and how each component of the mitral valve apparatus works together.
In this guide, we’ll review mitral valve anatomy step by step, with a focus on the mitral valve leaflets, segments, commissures, and supporting structures so you can recognize what you are seeing on TTE and TEE and describe it with clarity.
Mitral Valve Function
Before we break down mitral valve anatomy, let’s first review what the mitral valve is designed to do.
The mitral valve regulates blood flow in three important ways:
1. Promotes forward flow during diastole
When the left ventricle relaxes, the mitral valve opens and allows blood to move from the left atrium into the left ventricle.
2. Prevents backflow during systole
When the left ventricle contracts, the mitral valve closes to prevent regurgitation of blood back into the left atrium.
3. Supports left ventricular geometry and function
The mitral valve apparatus is physically connected to the left ventricle through the chordae tendineae and papillary muscles. Because of this connection, it plays a key role in maintaining ventricular shape and coordinated contraction. Changes in ventricular size or function can directly affect mitral valve competence.
This is why mitral valve disease is rarely isolated to the leaflets alone. Ventricular dilation, papillary muscle displacement, or annular enlargement can all disrupt normal valve function.
Understanding mitral valve function first makes it much easier to appreciate how each component of the mitral valve apparatus contributes to overall valve competence.
The Mitral Valve Apparatus
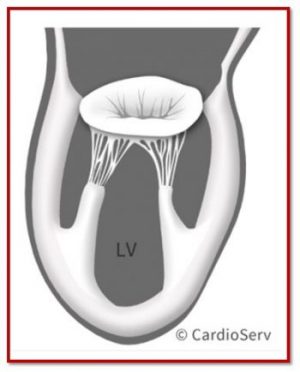
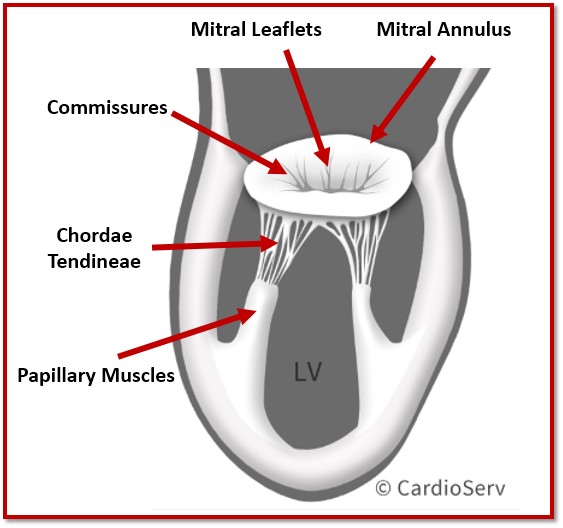
The mitral valve is more than just two leaflets opening and closing. It is a dynamic structure known as the mitral valve apparatus, and every component must function together to maintain proper blood flow from the left atrium to the left ventricle.
The mitral valve apparatus consists of five main parts:
- Mitral annulus
- Anterior and posterior mitral valve leaflets
- Commissures
- Papillary muscles
- Chordae tendineae
Each structure plays a specific role in valve competence. When one component is abnormal, the entire system is affected.
For sonographers, it’s important to think of the mitral apparatus as a functional unit rather than isolated parts. For example, mitral regurgitation may not be caused by a leaflet problem alone. Annular dilatation, papillary muscle displacement, or chordal rupture can all disrupt normal leaflet coaptation.
Understanding the mitral valve apparatus helps you:
- Recognize primary versus functional mitral regurgitation
- Accurately identify mitral valve segments
- Describe pathology clearly in your report
- Communicate effectively with interpreting physicians
Before we break down each structure individually, remember this key concept: normal mitral valve function depends on alignment, support, and coordinated motion throughout the cardiac cycle.
When that coordination is lost, pathology develops.
1. Mitral Annulus
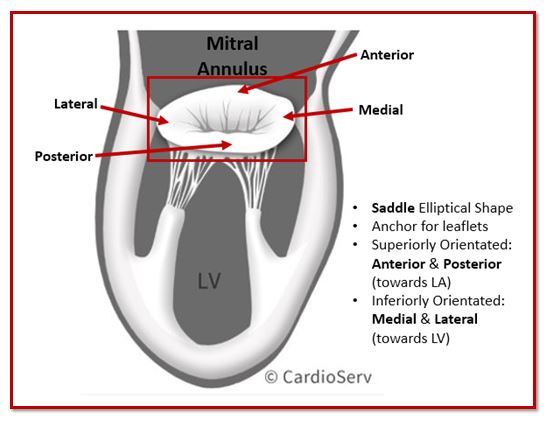
The mitral annulus forms the structural foundation of the mitral valve apparatus. It is a fibrous ring that anchors the anterior and posterior mitral valve leaflets and maintains valve geometry throughout the cardiac cycle.
Although often described as a simple ring, the mitral annulus is actually saddle-shaped and dynamic. Its three-dimensional shape changes during systole and diastole to help maintain proper leaflet coaptation.
Key Features of the Mitral Annulus
- Saddle-shaped configuration
- Anterior portion in fibrous continuity with the aortic valve
- Posterior portion more muscular and prone to dilation
- Dynamic size and shape changes during the cardiac cycle
This dynamic behavior is important. During systole, the annulus contracts and deepens its saddle shape, helping the leaflets coapt effectively. In diastole, it enlarges to facilitate forward blood flow into the left ventricle.
2. Mitral Leaflets
The mitral valve consists of two primary leaflets:
- Anterior leaflet
- Posterior leaflet
While this sounds simple, accurate identification of mitral valve leaflets and segments is essential for describing pathology correctly on echocardiography.
Anterior Mitral Valve Leaflet
The anterior leaflet is larger and more triangular in shape. It occupies approximately one third of the annular circumference but has a greater surface area than the posterior leaflet.
It is in fibrous continuity with the aortic valve, forming part of the aorto-mitral curtain. Because of this structural relationship, pathology involving the anterior leaflet may also affect left ventricular outflow tract dynamics.
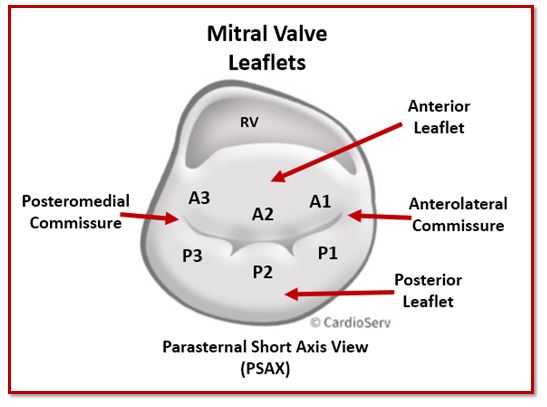
For segmentation purposes, the anterior leaflet is divided into:
- A1 – lateral scallop
- A2 – middle scallop
- A3 – medial scallop
Posterior Mitral Valve Leaflet
The posterior leaflet is shorter in height but spans a larger portion of the annulus. It is divided into three distinct scallops, which are often more clearly separated than those of the anterior leaflet:
- P1 – lateral scallop
- P2 – middle scallop
- P3 – medial scallop
The posterior leaflet is most commonly involved in degenerative mitral valve disease, particularly P2 prolapse.
3. Commissures
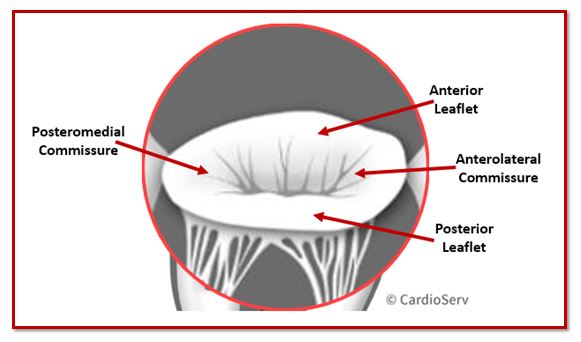
The commissures are the junctional areas where the anterior and posterior mitral valve leaflets meet. They mark the transition between the leaflets and help define the boundaries of the mitral valve segments.
There are two commissures:
- Anterolateral commissure
- Posteromedial commissure
Understanding their location is essential for accurate segment identification and clear reporting.
Anterolateral Commissure
The anterolateral commissure lies between:
- A1 and P1 scallops
It is positioned closer to the lateral wall of the left ventricle. The anterolateral papillary muscle provides chordal support to this region.
Posteromedial Commissure
The posteromedial commissure lies between:
- A3 and P3 scallops
This region is supplied by the posteromedial papillary muscle, which typically has a single coronary blood supply. Because of this, the posteromedial commissure is more vulnerable to ischemic injury following myocardial infarction.
4. Chordae Tendineae
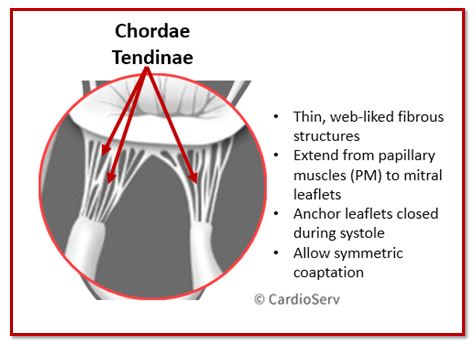
The chordae tendineae are fibrous cords that connect the mitral valve leaflets to the papillary muscles. They act as tension-support structures, preventing the leaflets from prolapsing into the left atrium during systole.
Without properly functioning chordae, the mitral valve cannot maintain effective coaptation.
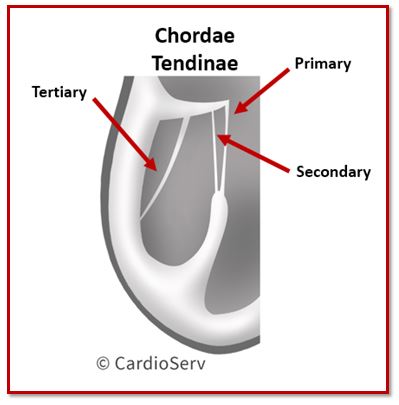
Structure of the Chordae Tendineae
Chordae originate from the papillary muscles and insert into the ventricular surface of the mitral valve leaflets.
They are typically classified into three groups:
- Primary chordae – attach to the free edge of the leaflets and prevent prolapse
- Secondary chordae – attach to the ventricular surface of the leaflet body and help distribute mechanical stress
- Tertiary chordae – found primarily on the posterior leaflet and attach directly to the ventricular wall
Each leaflet receives chordal support from both papillary muscles, creating a balanced suspension system.
Functional Importance
During systole, left ventricular contraction pulls on the papillary muscles, which in turn tension the chordae tendineae. This coordinated movement stabilizes the mitral valve leaflets and prevents them from inverting into the left atrium.
If the chordae are:
- Ruptured → flail leaflet and acute mitral regurgitation
- Elongated → leaflet prolapse
- Restricted or tethered → functional mitral regurgitation
Because the chordae are directly influenced by left ventricular geometry, ventricular dilation or ischemia can significantly impact mitral valve function even when the leaflets themselves are structurally normal.
5. Papillary Muscles
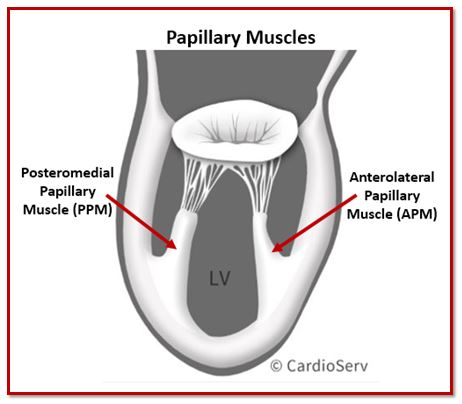
The papillary muscles are the final component of the mitral valve apparatus and play a critical role in valve stability. These muscular projections arise from the left ventricular wall and anchor the chordae tendineae, which in turn support the mitral valve leaflets.
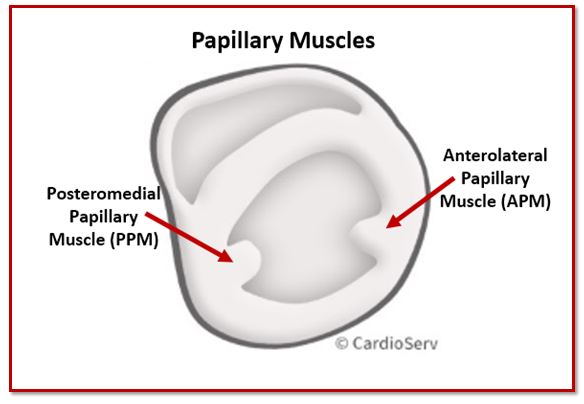
There are two papillary muscles:
- Anterolateral papillary muscle
- Posteromedial papillary muscle
Each papillary muscle sends chordae to both mitral valve leaflets, creating a balanced suspension system that maintains proper leaflet alignment during systole.
Anterolateral Papillary Muscle
The anterolateral papillary muscle typically has a dual blood supply from the left anterior descending and circumflex arteries. Because of this dual supply, it is less commonly affected by isolated ischemic events.
Posteromedial Papillary Muscle
The posteromedial papillary muscle usually has a single coronary blood supply, most often from the right coronary artery or left circumflex depending on dominance.
This single blood supply makes it more vulnerable to ischemia or infarction. Papillary muscle dysfunction or rupture in this region can lead to acute, severe mitral regurgitation.
Functional Importance
During systole, left ventricular contraction causes the papillary muscles to contract simultaneously. This coordinated movement tensions the chordae tendineae and stabilizes the mitral valve leaflets, preventing prolapse into the left atrium.
When papillary muscles are:
- Displaced due to ventricular dilation
- Dysfunctional from ischemia
- Ruptured following myocardial infarction
The result can be leaflet tethering, poor coaptation, or acute flail segments.
This is why mitral valve disease often reflects ventricular pathology rather than isolated leaflet abnormalities.
Mitral Valve Zones
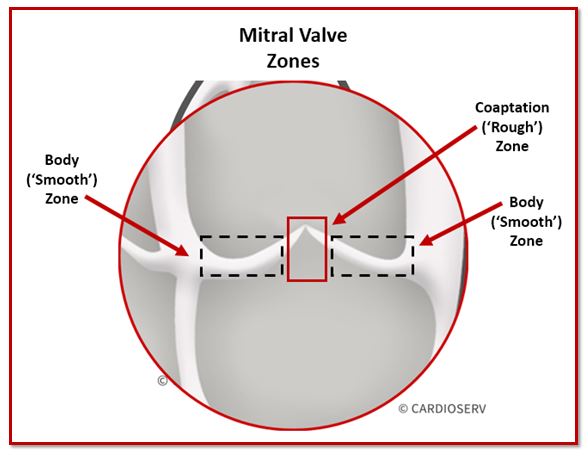
The mitral valve apparatus includes subtle structural details that become important when describing pathology precisely. When we zoom in on the mitral valve leaflets from the atrial surface, two functional zones can be identified.
These zones help localize where abnormalities occur.
1. Body (“Smooth”) Zone
The body zone refers to the smooth surface area of the leaflet. This region:
- Forms the majority of the leaflet body
- Is relatively thin and flexible
- Does not directly participate in leaflet coaptation
Pathology involving the smooth zone may include thickening, calcification, or degenerative changes affecting leaflet mobility.
2. Coaptation (“Rough”) Zone
The coaptation zone, also known as the rough zone, represents the portion of the leaflet that directly meets the opposing leaflet during systole.
This region:
- Contains chordal insertions
- Is slightly thicker
- Is the critical contact area responsible for valve competence
Because proper coaptation is essential for preventing mitral regurgitation, this zone is a crucial area to observe during echo assessment.
Key Tips to Take Away
- Always evaluate all components of the mitral valve apparatus, not just the leaflets.
- Scallop visualization can vary depending on scanning window and probe angulation. Confirm segment identification in multiple views.
- The posterior leaflet is more prone to prolapse and remodeling than the anterior leaflet.
- Scallops are labeled from lateral to medial:
A1/P1 → A2/P2 → A3/P3. - Papillary muscle support follows this pattern:
Anterolateral → lateral scallops (A1, P1) and lateral half of A2/P2
Posteromedial → medial scallops (A3, P3) and medial half of A2/P2. - Chordae tendineae are essential for maintaining proper leaflet coaptation and overall mitral valve function.
Ready to take this a step further?
If scallop orientation or probe angulation ever feels confusing, this visual guide was built to simplify it.
Master Mitral Valve Imaging with Confidence
A Practical Visual Guide for Sonographers
A step-by-step visual guide to scallop identification, echo orientation, and mitral valve imaging in TTE and TEE.
- ✔ Confidently identify scallops in TTE and TEE
- ✔ Understand echo orientation from sonographer vs surgeon view
- ✔ Optimize imaging windows and probe angulation
- ✔ Dozens of labeled echo diagrams for quick reference

Andrea Fields MHA, RDCSStay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Prokšelj, K. (2015). Echocardiography Of The Mitral Valve. International Symposium MITRAL VALVE DISEASES IN CHILDREN AND ADULTS. doi:10.5644/pi2017.168.03
Zoghbi, W. A., MD, Adams, D., RCS, RDCS, FASE, & Bonow, R. O., MD. (2017). Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation. JASE,30(4), 318-334. Retrieved June 6, 2017. DOI: 10.1016/j.echo.2017.01.007
Zamorano, J. L., MD, & Badano, L. P. (2011). EAE/ASE Recommendations for the Use of Echocardiography in New Transcather Interventions for Valvular Heart Disease. JASE,24(9), 957-960. Retrieved June 6, 2017. DOI: 10.1016/j.echo.2011.07.003