Last Updated on November 18, 2025 by Don Gerig, RDCS
Last week, in Part 1 of our series on the 2025 ASE Right Heart Guidelines, we highlighted the shift from diagnosis to prognosis.
This week, we’re focusing on the most significant updates to the 2025 ASE Right Heart new severity grading, and what they mean for your echo lab.
It has been over a decade since the ASE last updated its recommendations for evaluating the right heart. Since then, our understanding of pulmonary hypertension (PH) and right heart function has advanced significantly.
The 2025 ASE Right Heart new severity gradings reflect this progress, moving us from single cutoffs to graded severity and from isolated numbers to integrated probability models, using a three-pillar model: STRUCTURE – FUNCTION – HEMODYNAMICS. The result? Clearer, more consistent standards for sonographers and physicians.
Top 5 Changes to the 2025 ASE Right Heart Guidelines
1. Pulmonary Hypertension: Lower Diagnostic Threshold
- Pulmonary Hypertension: Previously described as mPAP >25 mmHg on right heart catheterization. Updated to:
- Pulmonary Hypertension: Mean Pulmonary Artery Pressure (mPAP): >20 mmHg, aligning with the World Symposium on PH.
Why it matters: Even mild elevations in pulmonary pressure carry prognostic significance. By lowering the threshold, patients can be recognized and monitored earlier. The new guidelines emphasize that echocardiography does not diagnose PH, but instead assigns probability based on tricuspid regurgitant velocity (TRV) and supportive findings.
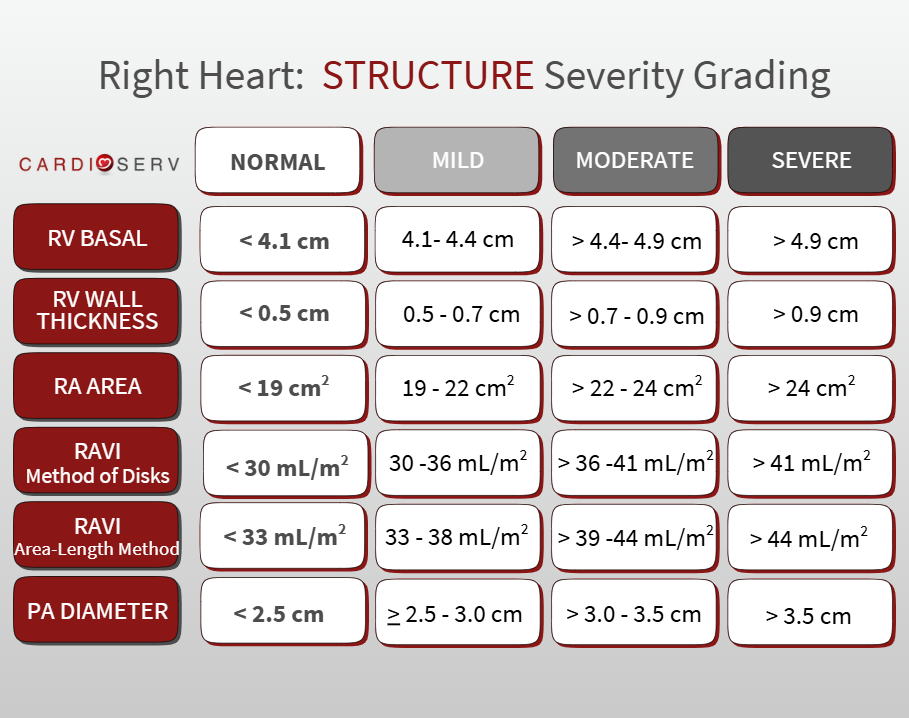
2.STRUCTURE: RA, RV, PA Size. From Single Cutoffs to Severity Grading
- RV Basal Diameter: Previously a single abnormal cutoff (>4.2 cm). Now graded into severity ranges for more nuanced reporting.
- Normal: < 4.1 cm
- Mild: 4.1–4.4 cm
- Moderate: >4.4–4.9 cm
- Severe: >4.9 cm
- RV Wall Thickness: Normal remains ≤0.5 cm. Now broken into severity ranges.
- Normal: < 0.5 cm
- Mild: 0.5–0.7 cm
- Moderate: >0.7–0.9 cm
- Severe: >0.9 cm
- RA Area: No longer a simple “>18 cm² = abnormal.” The 2025 guidelines now grade RA area into mild, moderate, and severe enlargement.
- Normal: < 19 cm²
- Mild: 19–22 cm²
- Moderate: >22–24 cm²
- Severe: >24 cm²
- RA Volume Index (RAVi): New cutoffs introduced for the first time in 2025. Method of Disks is the preferred calculation method for RAVi but Area-Length Method can be used if your equipment cannot calculate area with Method of Disks.
- Method of Disks (Preferred Calculation)
- Normal: < 30 mL/m²
- Mild: 30–36 mL/m²
- Moderate: >36–41 mL/m²
- Severe: >41 mL/m²
- Area-Length Method
- Normal: < 33 mL/m²
- Mild: 33–38 mL/m²
- Moderate: 39–44 mL/m²
- Severe: >44 mL/m²
- Pulmonary Artery (PA) diameter: Reaffirmed as supportive for PH, now reported with graded severity ranges.
- Normal: < 2.5 cm
- Mild: 2.5 – 3.0 cm
- Moderate: > 3.0 – 3.5 cm
- Severe: > 3.5 cm
- PA-to-Aorta (PA/Ao) Ratio: Introduced in 2025 as a supportive marker for PH.
- Abnormal if ≥ 1.0
Why it matters: Rather than labeling enlargement simply as “abnormal,” clinicians can now grade severity. This improves risk stratification and allows for better tracking of disease progression over time.
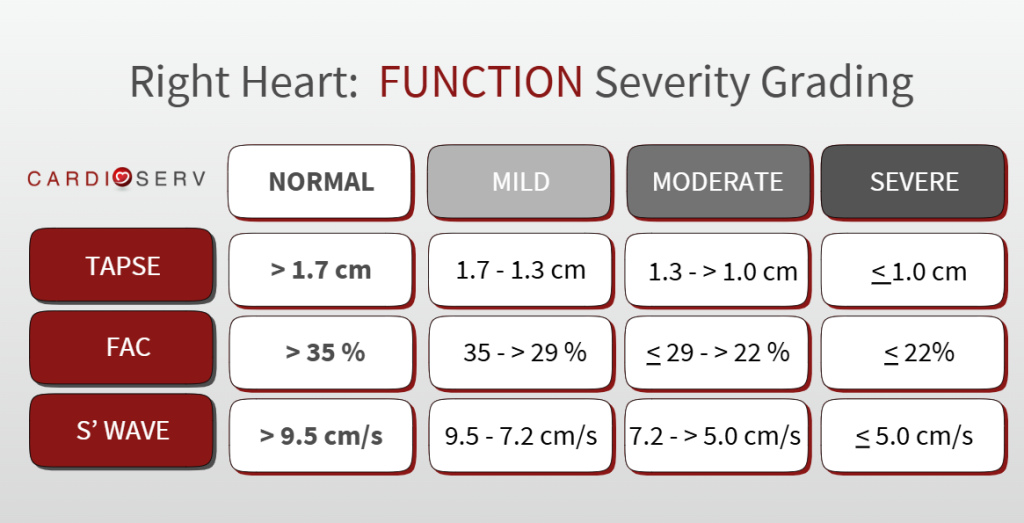
3. FUNCTION: TAPSE and FAC Severity Grading
- TAPSE: cutoff unchanged (>1.7 cm = normal), but now graded into mild, moderate, and severe dysfunction for more precise reporting.
- Mild: 1.7–1.3 cm*
- Moderate: 1.3–1.0 cm
- Severe: <1.0 cm
- FAC: Formerly just “<35% = abnormal.” In 2025, FAC now has graded severity ranges
- Mild: ≤35% to >29%
- Moderate: ≤29% to >22%
- Severe: ≤22%
- S′ Velocity: Prior binary cutoff value of <9.5 cm/s abnormal. 2025 ASE Guidelines provide severity grading.
- Normal: > 9.5 cm/s
- Mild: 9.5 – 7.2 cm/s**
- Moderate: 7.2- > 5.0 cm/s
- Severe: < 5.0 cm/s
Why it matters: Right ventricular (RV) systolic function is no longer binary (normal or abnormal). By grading TAPSE and FAC, echocardiography reports can now communicate the degree of dysfunction, enhancing prognostic accuracy and consistency across labs.
*Note: TAPSE 1.3 cm is graded as both mild and moderate per ASE Guidelines, **Note: S’ Wave 7.2 cm/s is graded as both mild and moderate per ASE Guidelines.
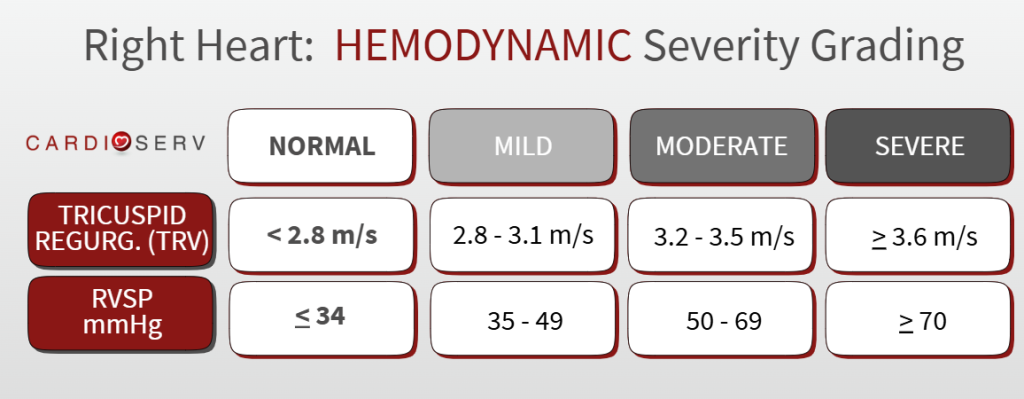
4. HEMODYNAMICS: TRV Updated Standards
- Tricuspid Regurgitant Velocity (TRV): now graded normal, mild, moderate, severe.
- Normal: < 2.8 m/s
- Mild: 2.8–3.1 m/s
- Moderate: 3.2–3.5 m/s
- Severe: >3.6 m/s
- RAP Estimation: Continued emphasis on reporting specific values based on the collapsibility index (3, 8, or 15 mmHg).
- RVSP (Right Ventricular Systolic Pressure): New reference ranges and clarity on severity grading
- Normal: < 34mmHg
- Mild: 35 – 49 mmHg
- Moderate: 50 – 69 mmHg
- Severe: > 70 mmHg
Why it matters: These refinements sharpen the probability model for pulmonary hypertension. Standardizing TRV grading and PA measurements improve reproducibility across echo labs providing physicians with more confidence in both the diagnosis and prognosis of pulmonary hypertension.
5. New Emphasis on RV Strain and 3D Measurements
- RV Longitudinal Strain: Emphasis on RV free wall strain with severity grading. This allows earlier detection of RV dysfunction and carries strong prognostic value.
- 3D RA and RV Volumes Indexed to BSA: Preferred when available, as 3D reduces geometric assumptions and improves accuracy, especially in irregularly shaped chambers.
Why it matters: RV strain and 3D volumes correlate more closely with outcomes than TAPSE or FAC alone. If your lab has the technology, incorporating these advanced tools enhances precision and reproducibility.
Looking Ahead
The 2025 ASE Right Heart Guidelines represent the most comprehensive update in over a decade. With a lower diagnostic threshold for pulmonary hypertension and graded severity cutoffs for chamber size and function, echocardiography now provides a clearer and more reliable picture of right heart performance.
And we’re just getting started. Next week in Part 3, we’ll take a deep dive into one of the most widely used—and often misused—parameters of RV systolic function: TAPSE. We’ll explore how the 2025 guidelines reframe its role, the correct way to measure it, and why it should never be interpreted in isolation.
References
Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39.e14. doi:10.1016/j.echo.2014.10.003
Mukherjee M, Rudski LG, Addetia K, et al. Guidelines for the echocardiographic assessment of the right heart in adults and special considerations in pulmonary hypertension: Recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr. 2025;38(3):141-186. doi:10.1016/j.echo.2025.01.006

Don Gerig, RDCS Medical Education Manager
Connect on LinkedIn