Last Updated on April 1, 2026 by Don Gerig, RDCS
In part one of our HCM series you learned key echocardiographic clues that should raise suspicion for hypertrophic cardiomyopathy.
In this article we’ll look at one of the more challenging aspects of scanning patients with obstructive hypertrophic cardiomyopathy: accurately differentiating LVOT vs Mitral Regurgitation in HCM.
Both produce high-velocity systolic jets and sometimes even overlap on the same tracing, making it difficult to differentiate, even for experienced sonographers.
The good news is there are reliable ways you can tell these two CW signals apart, and that’s exactly what we’ll cover in this article.
Understanding “The Why”
Before you ever drop a CW Doppler cursor, it’s important to understand both what you’re measuring and why it matters.
While LVOT obstruction and MR can create similar Doppler signals, they originate from completely different mechanisms. And if one is misinterpreted as the other, it can potentially have a huge negative impact on patient outcomes.
In cases of obstructive HCM, both the turbulent LVOT flow and MR can be present at the same time.
If you:
- Mistake MR for LVOT → you may overestimate obstruction
- Mistake LVOT for MR → you may miss clinically significant regurgitation
Those differences in origin are exactly why the Doppler envelopes behave differently.
These differences in origin are exactly why the Doppler envelopes behave differently. Understanding that physiology is what allows you to interpret the signal correctly.
A Moment to Pause
You’re scanning a patient with suspected HCM.
You place CW Doppler in the apical 5 chamber view and see a strong systolic signal. The velocity is high. The waveform looks abnormal.
This is the moment to pause.
Because this signal could represent:
- LVOT obstruction
- Mitral regurgitation
- Or both
Your next step determines whether you interpret it correctly.
Start With Physiology, Not Doppler
Before placing a Doppler cursor, take a step back and understand what you’re looking for.
LVOT Obstruction in HCM
- Caused by systolic anterior motion (SAM) of the mitral valve
- Creates a dynamic obstruction between the septum and mitral valve
- Flow accelerates progressively through systole as the obstruction dynamically worsens.
Mitral Regurgitation (MR) in HCM
- Caused by incomplete mitral valve closure
- Results in blood flowing back into the left atrium
- Begins earlier and often lasts longer in the cardiac cycle than LVOT flow
Understanding this difference is key because it directly explains the Doppler patterns you’ll see.
Different physiology → different Doppler patterns.
Let’s take a look at those differences next.
Key Doppler Differences: LVOT vs MR
There are four main clues that help separate LVOT obstruction from MR on Doppler:
- Shape of the envelope
- Timing of the signal
- Differences in velocity
- Direction of Flow
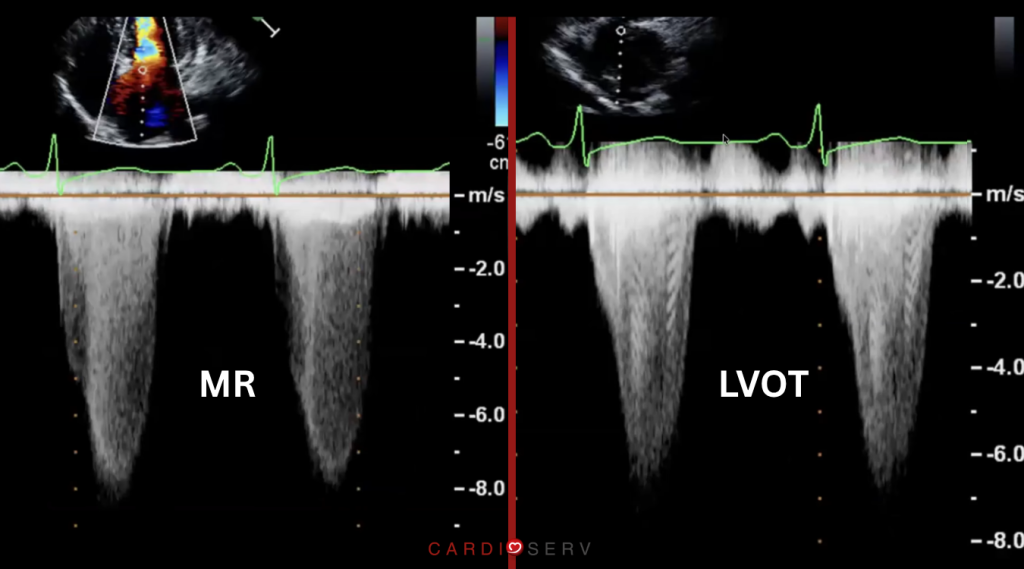
1. Shape of the Spectral Envelope
- LVOT Obstruction:
- Classic “dagger-shaped” appearance
- Narrow at the base, peaks late
- Reflects progressive acceleration during systole
- Mitral Regurgitation:
- More dense and broad signal
- Often more uniform throughout systole
- Does not have the same late-peaking pattern
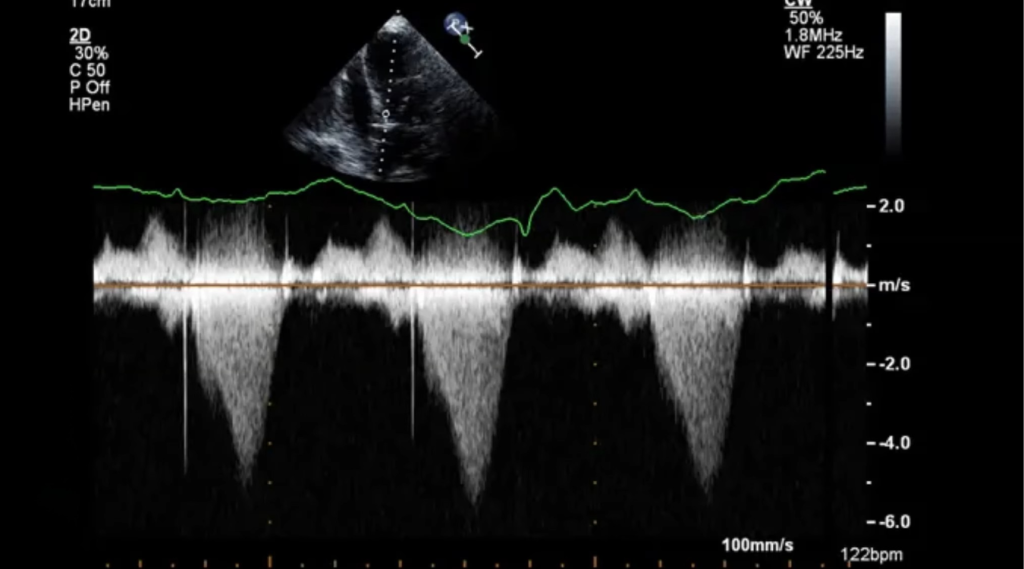
2. Timing of the Signal
This is actually one of the most reliable ways to differentiate the two.
- LVOT Obstruction:
- Begins after systole starts
- Typically peaks in mid-to-late systole
- Does not extend into isovolumic relaxation
- Mitral Regurgitation:
- Begins early in systole
- Often persists throughout systole
- Can extend into isovolumic relaxation
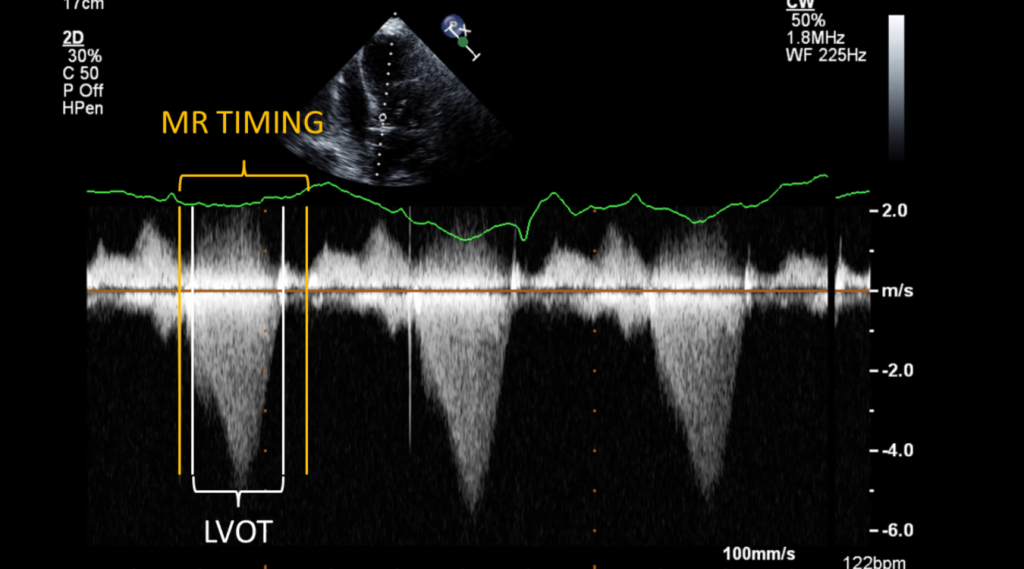
👉 If the signal continues beyond systole, you most likely looking at MR.
3. Velocity Differences
- MR jet velocity is almost always higher than LVOT velocity
Why?
Because MR reflects the pressure difference between the left ventricle and left atrium, which is greater than the pressure gradient between the left ventricle and the aorta.
👉 If you see two overlapping signals, the higher velocity jet is MR.
4. Direction of Turbulent Flow (Color Doppler Clues)
Before using spectral Doppler, always use color.
- LVOT flow: directed toward the aortic valve
- MR jet: directed into the left atrium
In SAM related MR, the MR jet is typically eccentric and posteriorly directed. You may even visualize multiple MR jets. Use your color Doppler to help differentiate and identify these multiple flow patterns before placing your Doppler cursor.
Common Pitfalls to Avoid
Chasing the Wrong Signal
This goes hand in hand with the last point we made above. Don’t blindly place your CW Doppler cursor without confirming flow direction. This can easily lead to incorrect measurements.
👉 Always identify the jet with color first. Then use your cursor.
Assuming One Signal = One Problem
In HCM, it’s common to have both LVOT obstruction and MR simultaneously.
If something doesn’t look right, consider that you may be seeing both and do what you can to differentiate the signals and measure correctly.
Tip: When chasing an LVOT gradient with CW, don’t worry about maintaining a good 2D image. Move your probe (and the patient) however you need to, to obtain the best angle of the LVOT and best Doppler signal.
This is especially true when scanning patients with sub-optimal image quality or while patients are performing valsalva. If you lose your image, it’s ok. Just be sure to verify the source of the Doppler before measuring or moving on.
Think you might be in MR flow? Check timing to verify.
Improper Cursor Alignment
Misalignment can:
- Underestimate velocities
- Blend signals together
- Make interpretation difficult
Be intentional with your cursor placement. Use color Doppler first to develop a plan of where to place the cursor. If the Doppler angle is too great, readjust and try to approach the flow from a lesser angle.
Ignoring Timing
If you’re not paying attention to when the signal occurs, you’re guessing.
Timing is one of your most powerful tools in these cases.
A Practical Step-by-Step Approach
When evaluating a patient with suspected HCM:
- Start with 2D imaging
• Look for septal hypertrophy
• Assess LV cavity size
• Look for SAM
• Look for hyperdynamic LV function - Add color Doppler
• Identify turbulence
• Determine direction of flow (MR vs LVOT flow)
• Determine number of MR jets and direction - Place CW Doppler intentionally
• Align with the LVOT first
• Then assess the MR jet separately
• Annotate each - Analyze the waveform carefully
• Shape
• Timing
• Peak velocity - Confirm your findings
• Does the timing, direction, and peak velocity make sense for the signal you think you’re measuring?
Putting It All Together
Obstruction is dynamic, so the key to differentiating LVOT from MR isn’t memorizing patterns, it’s first understanding the physiology and then applying a consistent approach, and a willingness to take the time necessary to accurately differentiate Doppler waveforms.
When you put all of the findings together, you move from guessing to confidently identifying the source of the Doppler signal.
What Comes Next
Now that you can differentiate LVOT obstruction from mitral regurgitation in HCM, the next step is learning how to unmask obstruction that isn’t visible at rest.
Because in many patients with HCM, the gradient isn’t always present until you provoke it.
In the next article, we’ll walk through how to use goal-directed Valsalva to uncover dynamic LVOT obstruction and improve diagnostic accuracy in your lab.
Ready to Go Even Deeper?
If you’ve ever questioned whether you were truly measuring LVOT flow or MR, our webinar brings these Doppler patterns to life with real case examples and side-by-side Doppler review.
If you’d like to see real case examples of:
- Real case examples of HCM in the echo lab
- LVOT vs MR differentiation
- Goal-directed Valsalva in action
- Differences between obstructive and non-obstructive HCM
- Access to Free downloadable resources for you and your lab

Don Gerig, RDCS, Medical Education Manager
Connect on LinkedIn




