Last Updated on December 17, 2025 by Don Gerig, RDCS
By now, you can confidently identify a true pericardial effusion and avoid the common mimics, which we covered in part 2 of our pericardial disease series.
But the next question, and the one that determines the most urgency, is:
“Is the fluid under pressure?”
Cardiac tamponade isn’t just about fluid, it’s about pressure.
A small effusion can be deadly if it’s acute and rapidly accumulating. That’s why recognizing the signs of tamponade before clinical collapse is crucial.
In this guide, we break down how to recognize cardiac tamponade by reviewing the classic echo findings, from 2D structural signs and Doppler abnormalities to the predictable progression of hemodynamic compromise.
What Tamponade Actually Is
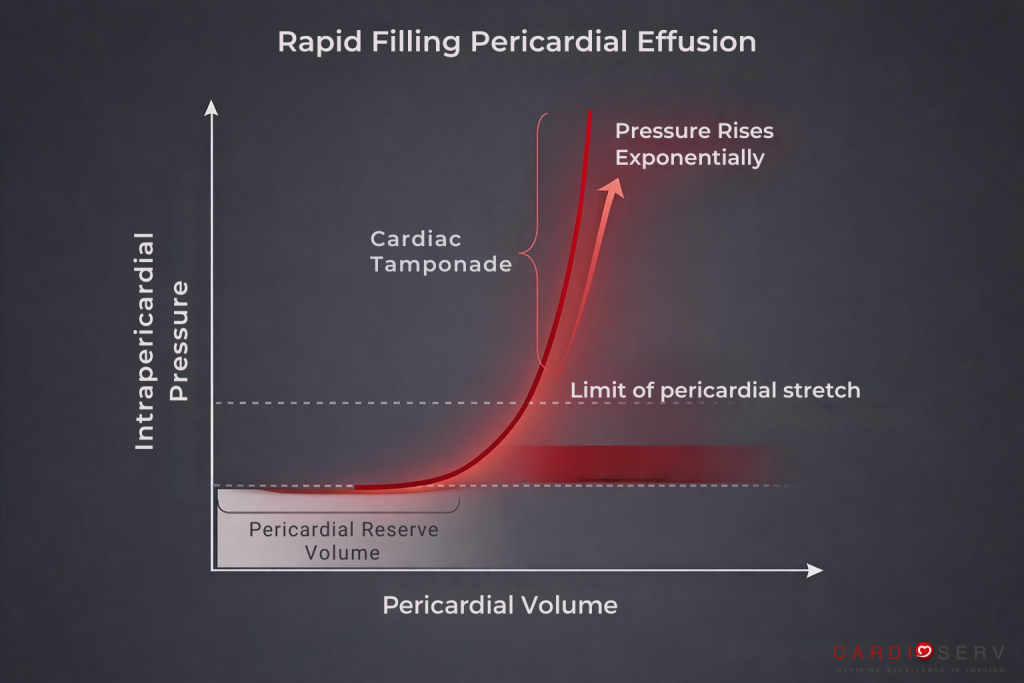
Tamponade occurs when intrapericardial pressure exceeds cardiac chamber pressures, impairing filling, especially during diastole. It is a pressure problem, not a fluid problem.
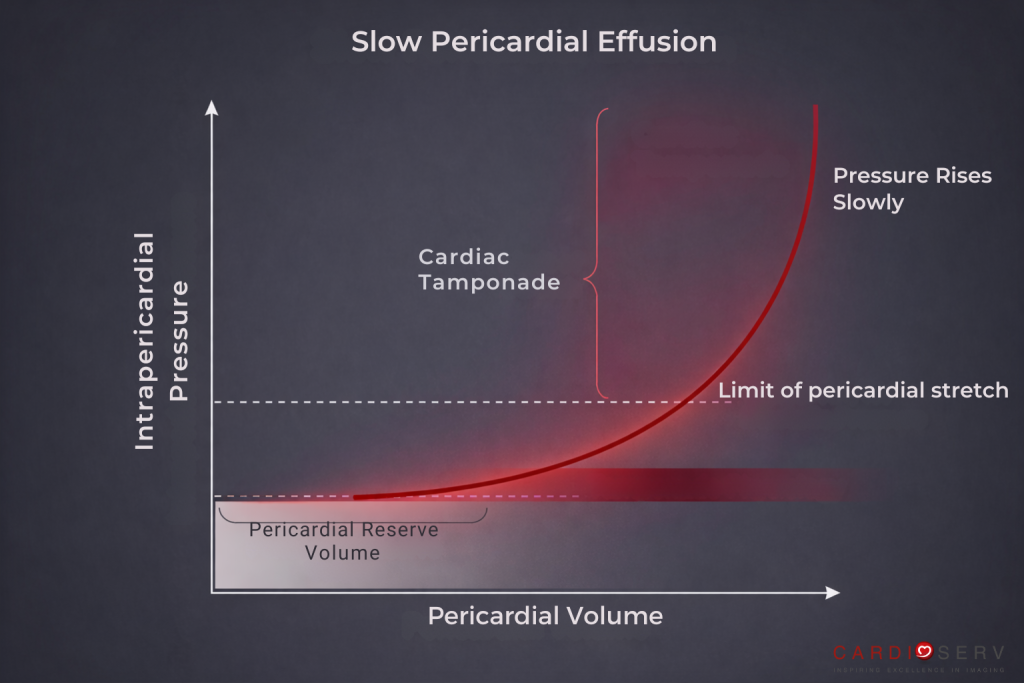
The pericardium can accommodate slowly accumulating fluid, but once its reserve volume is exceeded, the pressure-volume curve steepens dramatically (See diagram below):
- Small increases in fluid → large increases in intrapericardial pressure
- Diastolic chamber pressures are exceeded
- Chamber collapse occurs
- Cardiac output falls
This is why tamponade can occur with:
- Small but rapidly accumulating effusions (e.g., hemopericardium)
- Loculated or post-operative effusions (regional tamponade)
- Effusive-constrictive pericarditis
- Malignant or inflammatory processes in a non-compliant pericardium
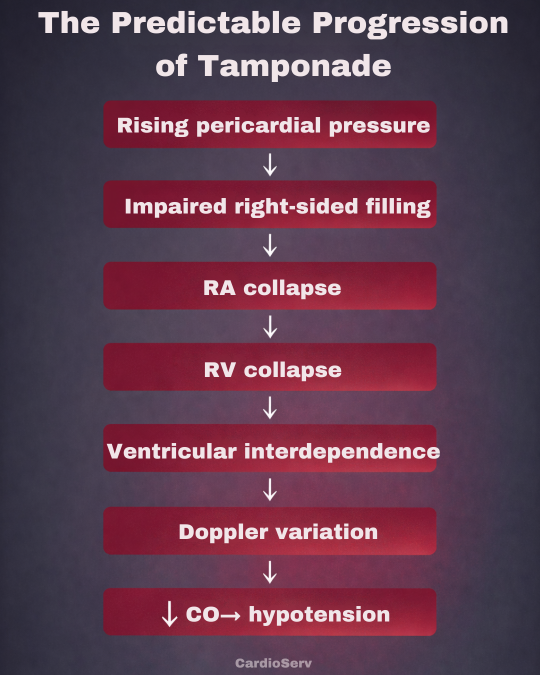
The Predictable Progression of Tamponade (Hemodynamic Cascade)
The progression of cardiac tamponade follows a predictable sequence of events:
- Rising pericardial pressure
- Impaired right-sided diastolic filling
- Right atrial collapse (late diastole)
- Right ventricular diastolic collapse (early diastole)
- Exaggerated ventricular interdependence
- Respiratory variation in mitral/tricuspid inflow
- IVC plethora (dilated, non-collapsible)
- ↓ Cardiac output → hypotension, tachycardia, pulsus paradoxus
Classic 2D Echo Signs of Cardiac Tamponade
Tamponade has reliable two-dimensional echo clues, some of which appear before clinical shock, enabling early recognition. Others, like LA/LV collapse or a “swinging heart,” often reflect more advanced or localized tamponade.
Right Atrial Collapse
- Occurs in late diastole when RA pressure is lowest.
- Sensitivity ~100 %, specificity ~80 %.
- Collapse lasting > ⅓ of the cardiac cycle is significant.
Right Ventricular Diastolic Collapse
- Occurs in early diastole when RV begins filling.
- Must time collapse to ECG or Doppler inflow to confirm diastolic timing.
- False positives: severe RV failure or hypovolemia.
Left Atrial (LA) Collapse
- Occurs in end-systole, typically affecting the posterior LA wall
- Seen in loculated, posterior, or postoperative effusions
- Specific but less sensitive (~25–30%)
- Important clue for regional tamponade or high posterior pericardial pressure
Left Ventricular (LV) Diastolic Collapse
- Collapse of the LV posterior wall during early diastole
- Indicates severe or loculated tamponade
- Rare, but highly specific when present
- Associated with malignant, posterior, or rapid-onset effusions
“Swinging Heart” Sign
- The heart appears to oscillate within a large effusion.
- Suggests high fluid volume but not always hemodynamic compromise.
IVC Plethora
- Dilated IVC > 21 mm with < 50 % collapse indicates elevated RA pressure.
In practice, RA and RV collapse are early signs of tamponade, while LA/LV collapse and a swinging heart typically appear later or in regional cases.
Doppler Clues: The Physiology in Motion
As intrapericardial pressure rises, each heartbeat becomes a pressure tug of war between the right and left sides of the heart.
- During inspiration: venous return increases to the right heart, but the stiff pericardium prevents expansion, so the septum shifts left and mitral inflow velocities drop.
- Expiration: The reverse occurs
This respiratory variation in Doppler inflow is a classic sign of tamponade physiology, reflecting impaired transmission of intrathoracic pressure into the cardiac chambers.
What To Look For With Doppler and Respiratory Variation
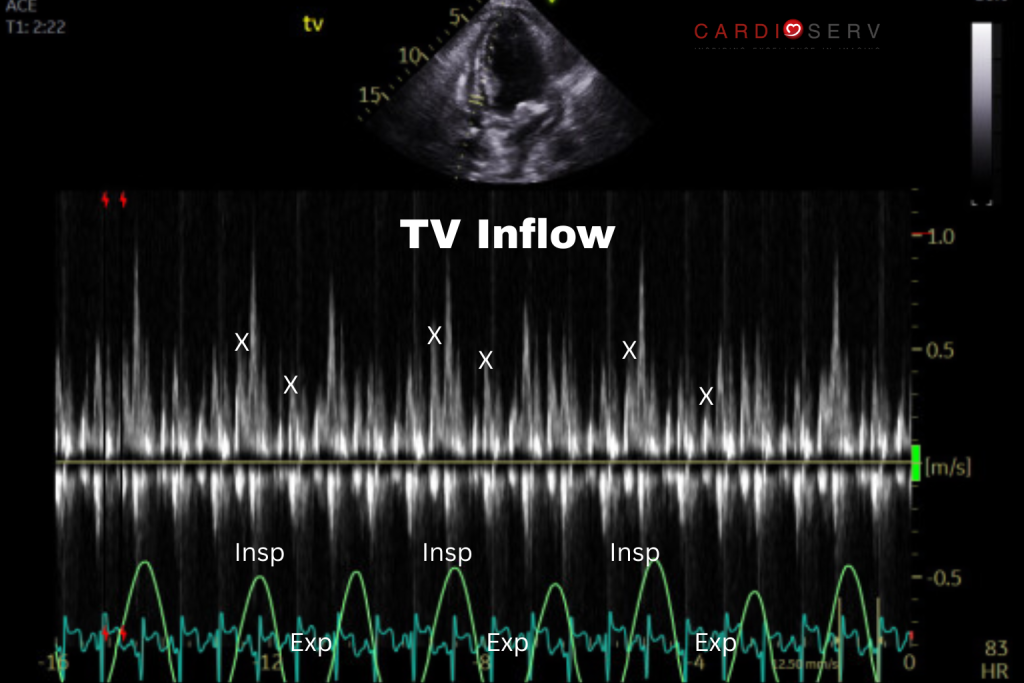
Tricuspid Valve Inflow
>60% increase of peak E wave velocity with inspiration, decrease with expiration.
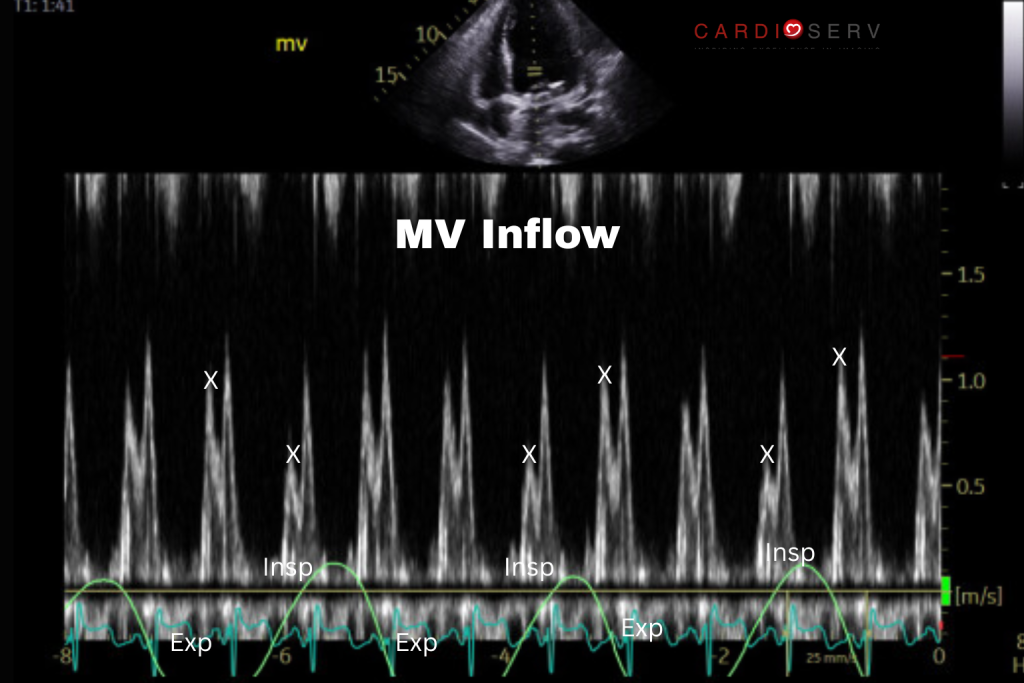
Mitral Valve Inflow
>30% decrease in peak E wave velocity with inspiration, increase with expiration.
How to Evaluate Respiratory Variation
Technique:
- View: Apical 4-chamber
- Mode: Pulsed-Wave Doppler
- Cursor position: At leaflet tips, parallel to flow
- Sweep speed: 25-50 mmHg (slow)
- Respiratory cycle: Label inspiration/expiration; record ≥3 full cycles
Hepatic Vein Doppler: The Confirmation Tool
The hepatic veins reflect RA pressure changes. In tamponade, elevated and unyielding pericardial pressure impairs normal venous return dynamics.
Use a subcostal view and place the Doppler sample 1–2 cm into the right or middle hepatic vein.
- Expiratory diastolic flow reversal occurs due to RA restriction
- Highly specific for tamponade physiology
- Reversal lasting >⅓ of cardiac cycle is diagnostic
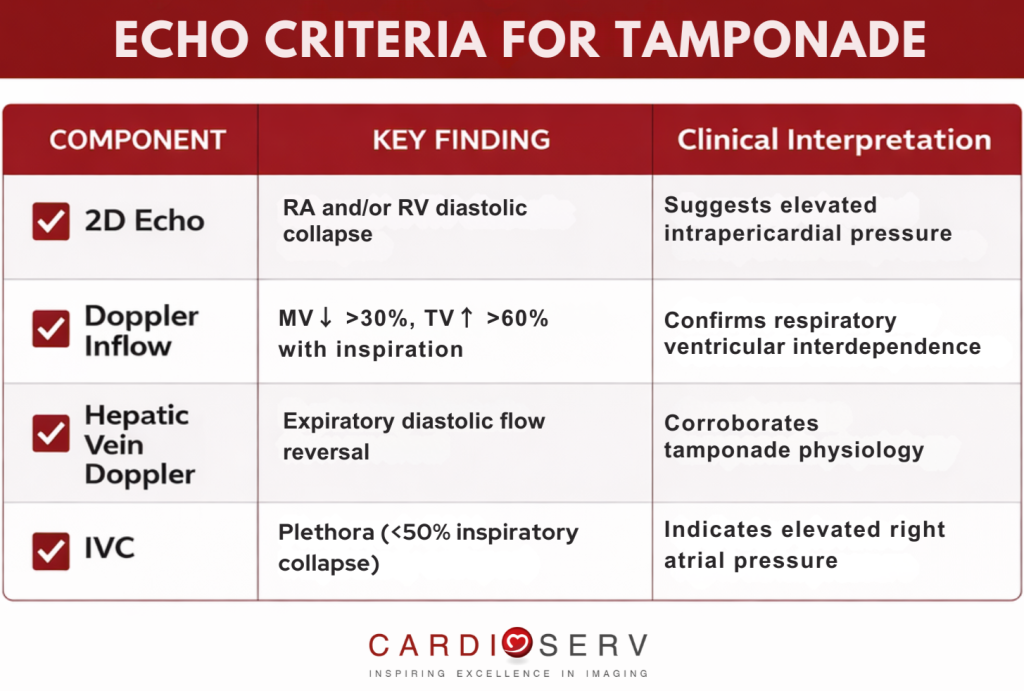
Putting It All Together
As we stated, tamponade physiology is not about how much fluid you see. It’s about rising pressure in the pericardial space that limits normal filling of the cardiac chambers.
These clues show up across different parts of the echo exam, including chamber motion, Doppler inflow patterns, and venous return. When you start to see that pattern come together, that’s when tamponade becomes likely.
If 3 out of these 4 criteria are present, tamponade physiology is highly likely, even in the absence of overt clinical collapse.
Tips and Pitfalls in Diagnosing Tamponade
Regional Tamponade
In postoperative patients or those with loculated effusions, the pericardial fluid may accumulate in only one region. These cases can cause regional tamponade, where classic signs like right atrial or ventricular collapse may be absent. In these cases, look for LA or LV collapse, or subtle Doppler changes. A high index of suspicion is key, especially in patients with recent cardiac surgery.
Hypovolemia or RV Infarct
In severely hypovolemic patients or those with right ventricular infarction, the RA and RV walls may appear collapsed simply due to low preload, not pericardial pressure. Always interpret collapse in the context of IVC size, Doppler variation, and the clinical picture, especially if the patient is fluid-depleted or hypotensive from another cause.
Constrictive Overlap
Sometimes, the pericardium may be both inflamed and stiff, leading to effusive-constrictive pericarditis. This can confuse the picture, as it shares features with tamponade (e.g., respiratory variation, IVC plethora) but also has constrictive features, such as:
- Annulus reversus or annulus paradoxus on tissue Doppler
- Septal bounce (reflecting ventricular interdependence)
- Hepatic vein diastolic reversal without IVC dilation
Pulsus Paradoxus
Pulsus paradoxus is an exaggerated drop in systolic blood pressure during inspiration (>10 mmHg) and is a classic sign of tamponade. It often mirrors what we see on Doppler, especially respiratory variation in mitral and tricuspid inflow. As sonographers, we don’t measure pulsus paradoxus directly, but we play a key role in confirming it by demonstrating these Doppler changes.
In Summary
Cardiac tamponade is a pressure problem, and echo is often the first to detect it. As sonographers, our role goes beyond image capture. By recognizing patterns like chamber collapse, Doppler variation, and IVC changes, we help identify tamponade before it leads to hemodynamic compromise. With thoughtful technique and a clear understanding of the physiology, we can help turn echo findings into actionable life-saving action.