In the last article of our pericardial disease series, we talked about how to identify cardiac tamponade with echo. For our final article of the series we’re taking a look at two conditions that can look a lot alike but require two very different treatments: constrictive pericarditis (CP) and restrictive cardiomyopathy (RCM).
Knowing how to differentiate these two conditions with echocardiography is a key skill to have since constrictive pericarditis can often be fixed with surgery, while restrictive cardiomyopathy is more about managing the underlying cause.
By the end of this article, you should be able to identify the echo findings most specific for constrictive physiology and recognize common pitfalls.
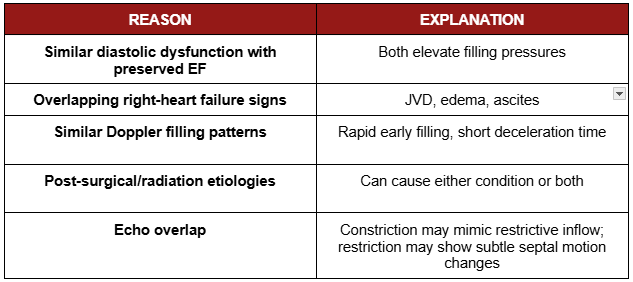
Quick Overview: Similar Symptoms, Different Causes
Both constrictive pericarditis and restrictive cardiomyopathy limit ventricular filling, but for completely different reasons.
They share nearly identical symptoms and often similar Doppler findings such as dyspnea, edema, JVD, preserved EF and abnormal filling, which is why they’re so commonly mistaken for one another.
But they arise from completely different mechanics, one from the outside of the heart, one from the inside.
Constrictive Pericarditis (CP): “The Squeeze from the Outside”
In constrictive pericarditis, a chronically thickened, fibrotic, or calcified pericardium loses its natural elasticity. Instead of stretching with each heartbeat, the pericardium becomes a rigid shell that mechanically restricts cardiac filling.
As venous return increases, the noncompliant pericardium halts further expansion. The result:
When one ventricle fills, the other is compressed, shifting the interventricular septum.
This phenomenon is called ventricular interdependence and it’s a hallmark of Constrictive Pericarditis.
Common Etiologies
Post-surgical (CABG, valve surgery)
Post-radiation therapy
Tuberculosis (especially in endemic regions)
Recurrent or viral pericarditis
Hemodynamic Hallmark of Constrictive Pericarditis
Constrictive Pericarditis is defined by abnormal pressure transmission:
In normal physiology, intrathoracic pressure changes with breathing are transmitted to the heart.
In constrictive pericarditis, that transmission is blocked which leads to “see-saw” respiratory variation in ventricular filling.
Inspiration: ↓ LV filling, ↑ RV filling
Expiration: the reverse
This exaggerated shift in diastolic flow is central to the diagnosis.
Restrictive Cardiomyopathy (RCM): “The Stiffness from Within”
In restrictive cardiomyopathy, the pericardium is healthy and normal. The problem is with the myocardium itself. The ventricular walls become abnormally stiff or infiltrated, which leads to impaired compliance and severely limited diastolic filling, even though the ejection fraction is oftentimes preserved.
Unlike constriction, the heart isn’t compressed from the outside. Instead, the muscle is intrinsically stiff:
Ventricular filling isuniformly impaired due to elevated myocardial stiffness or infiltration.
The pericardial sac is compliant, so there’s no exaggerated septal shift or ventricular interdependence.
Common Etiologies
Amyloidosis (most common cause in Western countries)
Hemochromatosis
Sarcoidosis
Post-radiation myocardial fibrosis
Endomyocardial fibrosis (more common in tropical regions)
Hemodynamic Hallmark of Restrictive Cardiomyopathy
Restrictive Cardiomyopathy produces high and equal diastolic pressures across chambers, but without significant respiratory variation:
Both ventricles fill poorly together
Tissue Doppler e′ velocities are reduced
Unlike constriction, there is no ventricular interdependence or “see-saw” filling pattern.
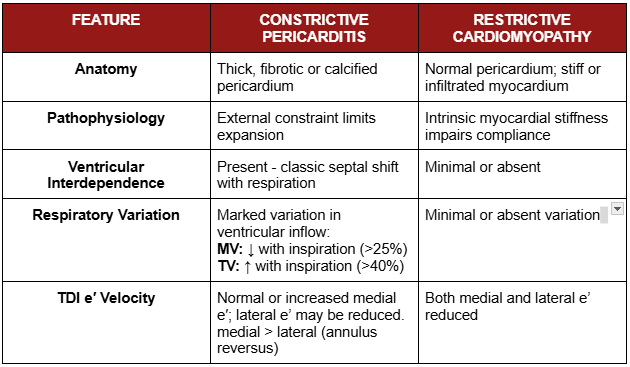
Constrictive Pericarditis vs Restrictive Cardiomyopathy: Key Echocardiographic Differences
2D and M-Mode Findings in Constrictive Pericarditis
Septal Bounce
Abrupt early-diastolic shift of the interventricular septum toward the LV
Reflects exaggerated ventricular interdependence
Best seen in apical 4-chamber or parasternal long-axis views
M-mode “shudder”
Shows rapid or notched motion of the septum in early diastole
Enhances detection when combined with ECG timing
Thickened/calcified pericardium
May appear echogenic on 2D imaging
Better characterized by CT or MRI
A normal appearing pericardium does not exclude constriction
IVC Dilatation and Hepatic Vein Variation
IVC ≥21 mm with <50% collapse → elevated RA pressure
Abnormal hepatic vein flow patterns
Doppler & TDI Findings in Constrictive Pericarditis – The Decisive Differentiators
Doppler inflow patterns and tissue velocities offer some of the clearest clues to tell the difference between Constrictive Pericarditis and Restrictive Cardiomyopathy.
Ventricular Inflow Variation
In constrictive pericarditis, exaggerated ventricular interdependence typically produces respiratory variation in ventricular inflow velocities.
Mitral inflow: decrease in peak E-wave velocity >25% with inspiration
Tricuspid inflow: increase in peak E-wave velocity >40% with inspiration
When present, these findings support constrictive physiology, particularly when they occur alongside abnormal septal motion, preserved tissue Doppler velocities, and systemic venous congestion.
Caused by impaired right atrial filling during expiration
Tissue Doppler Imaging (TDI) – “Annulus Reversus”
In constriction: medial e′ ≥ lateral e′
In restriction: both medial and lateral e′ are reduced
This reversal of expected e′ pattern (annulus reversus) is a key diagnostic marker of constrictive physiology.
Quick Summary of Echo Findings
CardioServ Tip:
Annulus reversus and respiratory inflow variation = think constriction
Globally reduced e′ and no ventricular inflow variation = think restriction
Common Pitfalls in Diagnosing Constrictive vs. Restrictive Physiology
Even experienced clinicians can misinterpret key findings when context or technique is suboptimal. Here’s how to recognize and avoid the most frequent diagnostic traps:
Why This Matters Clinically
Knowing how to distinguish constrictive pericarditis from restrictive cardiomyopathy is essential because the treatments differ dramatically.
Constrictive pericarditis is often surgically curable with pericardiectomy, while restrictive cardiomyopathy requires lifelong medical management of an underlying myocardial disease, such as amyloidosis or fibrosis.
Misdiagnosis can lead to delayed treatment, unnecessary surgery, or missed opportunities for targeted therapy. Mastering subtle echocardiographic clues like annulus reversus, septal bounce, and respiratory inflow variation can significantly impact patient outcomes.
Key Takeaways
Constrictive pericarditis is a disease of pericardial constraint, while restrictive cardiomyopathy is caused by intrinsic myocardial stiffness.
Ventricular interdependence is exaggerated in constriction, producing marked respiratory variation and septal motion tied to respiration.
Restrictive cardiomyopathy demonstrates impaired myocardial relaxation with relatively fixed septal behavior and minimal respiratory dependence.
Respiratory inflow variation values favor constrictive physiology, but must be interpreted within the broader echocardiographic pattern.
Tissue Doppler imaging is a key differentiator, with preserved or elevated medial e′ velocities favoring constriction and reduced e′ velocities favoring restriction.
Pitfalls and exceptions are common, particularly in elderly patients, mixed disease states, and postoperative or regional constriction.
References
Klein AL, Abbara S, Agler DA, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the Society for Cardiovascular Magnetic Resonance and Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. 2013;26(9):965-1012.e15. doi:10.1016/j.echo.2013.06.023
Mukherjee M, Rudski LG, Addetia K, et al. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults and Special Considerations in Pulmonary Hypertension: Recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr. 2025;38(3):141-186. doi:10.1016/j.echo.2025.01.006