Last Updated on November 6, 2025 by Don Gerig, RDCS
When evaluating mitral regurgitation on echo, color Doppler gives us the first visual clue, but it’s only the beginning of the story. To truly understand MR severity, we have to look beyond the jet and utilize spectral Doppler to assess the mitral regurgitation.
There are three Doppler techniques we can use, continuous-wave (CW), pulsed-wave (PW) at the mitral inflow, and PW of the pulmonary veins. With these three techniques for evaluating mitral regurgitation severity, we can piece together the hemodynamic puzzle and see how MR impacts both atrial and ventricular function.
Each Doppler tool tells part of the story: CW reveals velocity and contour, mitral inflow shows diastolic changes, and pulmonary veins reflect the atrial response. When interpreted together, they transform a color jet into a complete physiologic picture.
3 Doppler Techniques for Assessing Mitral Regurgitation
- CW Doppler MR Jet Velocity
- PW Doppler Mitral Valve Inflow
- PW Doppler of Pulmonary Veins
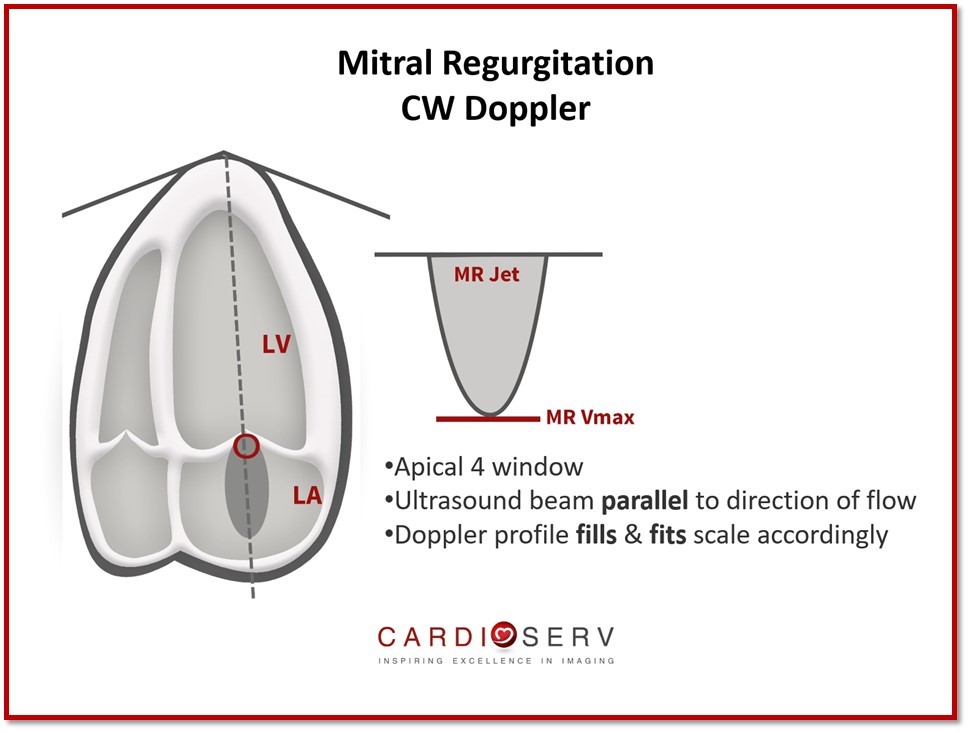
Continuous Wave (CW) Doppler MR Jet Velocity
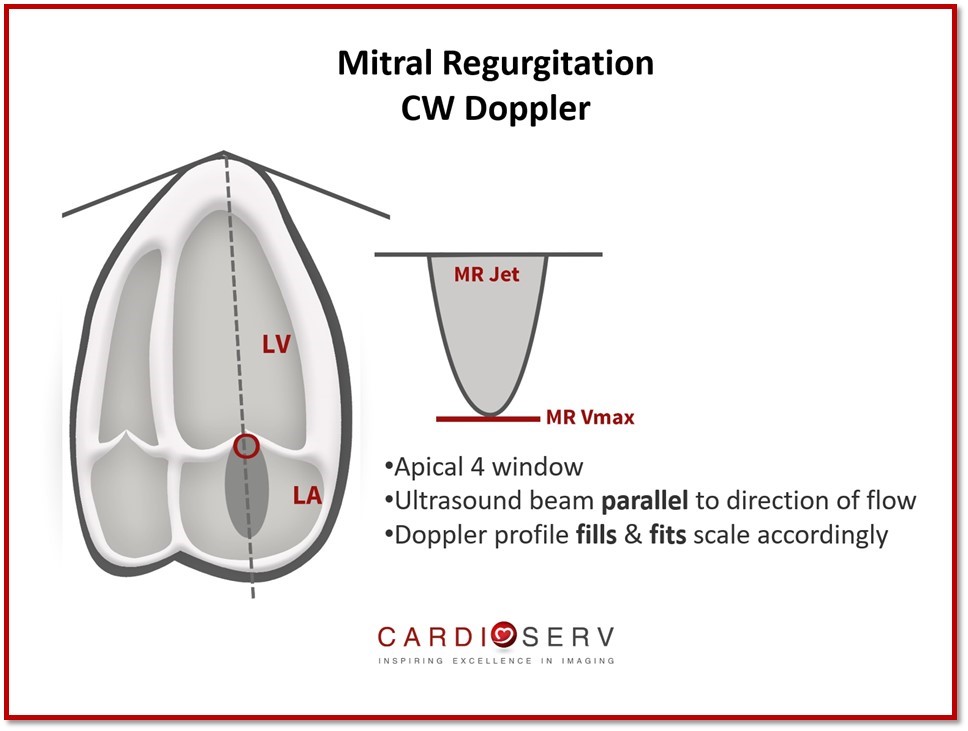
The profile of the Doppler jet can tell us a lot of information regarding hemodynamics and transvalvular flow rates. Even if MR is not detected with color Doppler, it is still essential to prove this with placing a CW Doppler through the mitral valve (MV) to demonstrate absence of flow below the baseline (TTE).
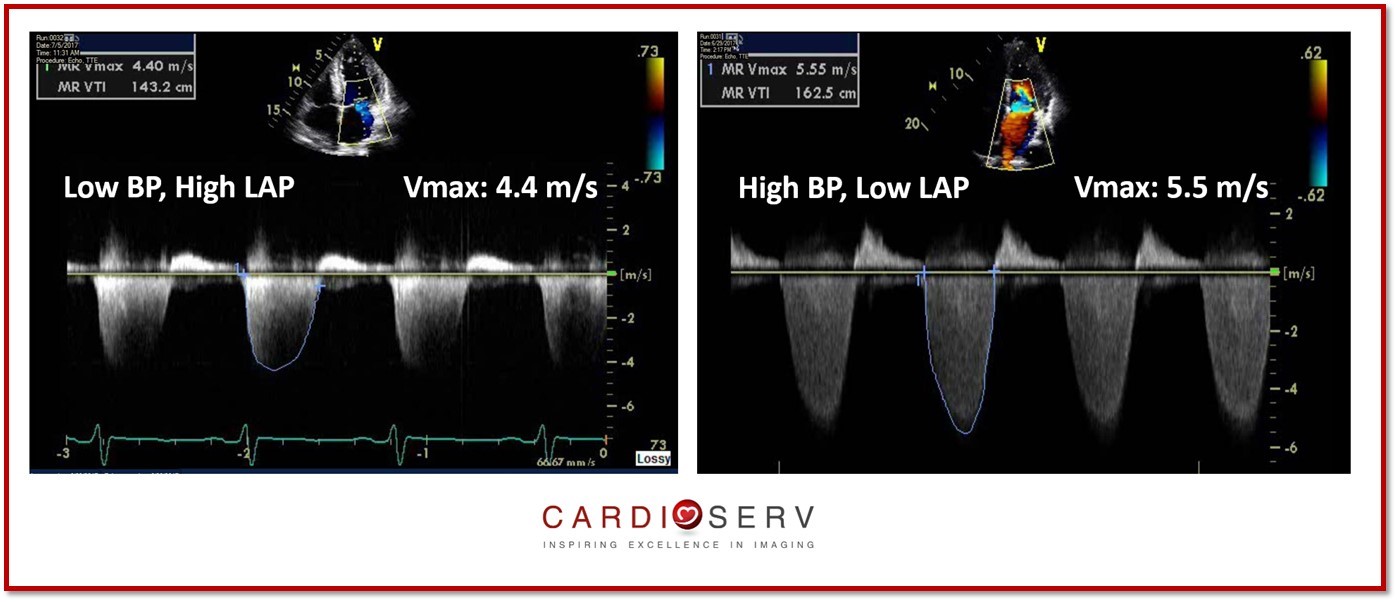
The max velocity of the MR jet does not provide us information on the severity of the MR. It does provide us with information regarding the hemodynamics of the LV & LA in regards to the MR. The max velocity of the jet represents the instantaneous systolic pressure gradient between the LV and LA.
It is common for the MR jet velocity to range between 4-6 m/s. This can allow us to easily analyze different scenarios:
- MR Vmax 4 m/s : indicate a low BP and high LAP
- MR Vmax 6 m/s : indicate a high BP and low LAP
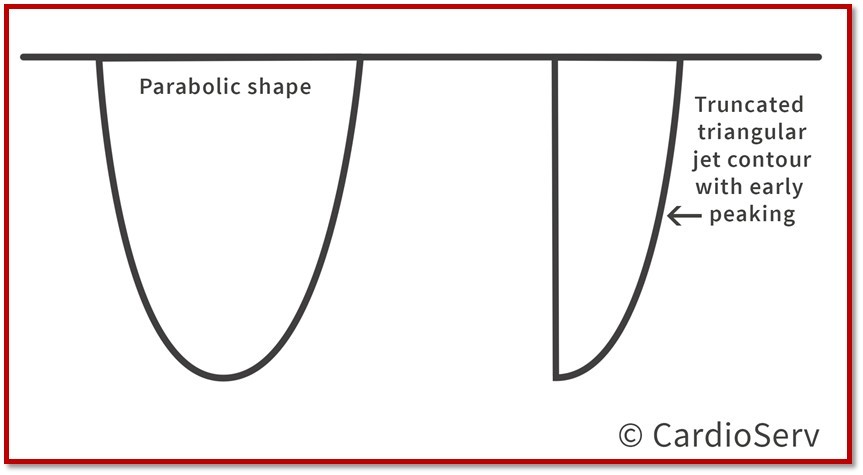
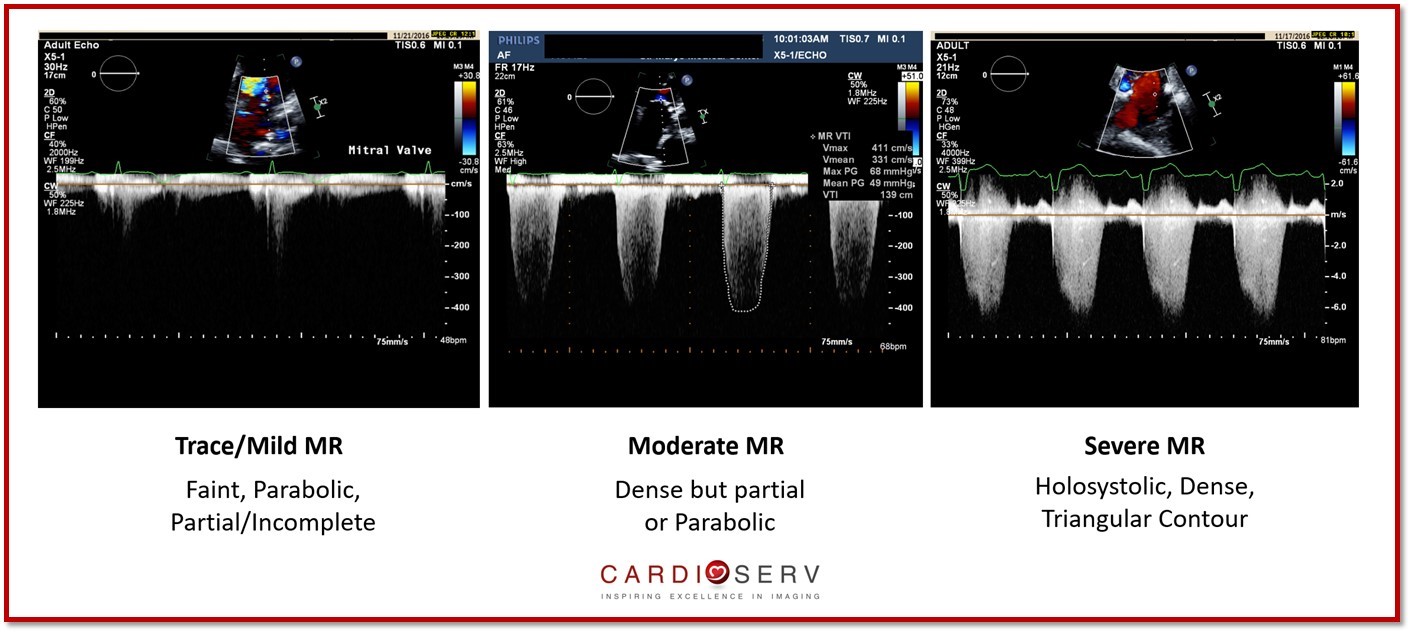
The contour and density of the jet can also provide qualitative information.
- Contour: aids in identifying the severity of MR
- Density: represents the number of RBC’s in the signal (amplitude & intensity)
Pulse Wave (PW) Doppler Mitral Valve Inflow
The inflow pattern and velocity can help us identify supportive signs of severe MR!
- Apical 4 window
- Ultrasound beam parallel to direction of flow
- Doppler profile fills & fits scale accordingly
- Gains adjusted for optional imaging
This velocity informs us of the forward stroke volume (SV) across the mitral valve. It can be increased if regurgitation is present.
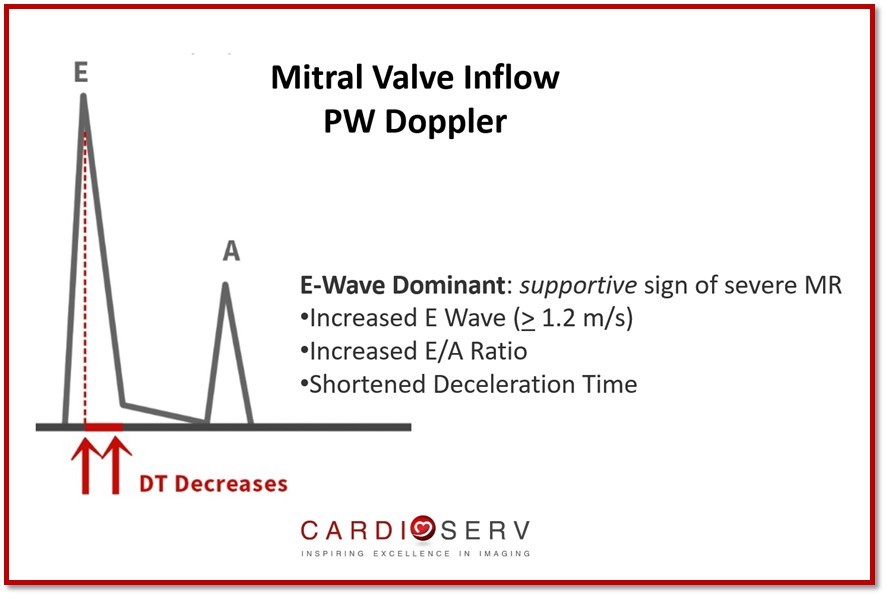
- E-Wave Dominant: supportive sign of severe MR
- Increased E Wave (> 1.2 m/s)
- Increased E/A Ratio
- Shortened Decel Time
- Reliable to assess primary MR
- Challenge for secondary
- Unable to differentiate between LV filling pressures or regurgitation
- Dominant A-Wave inflow pattern excludes severe MR
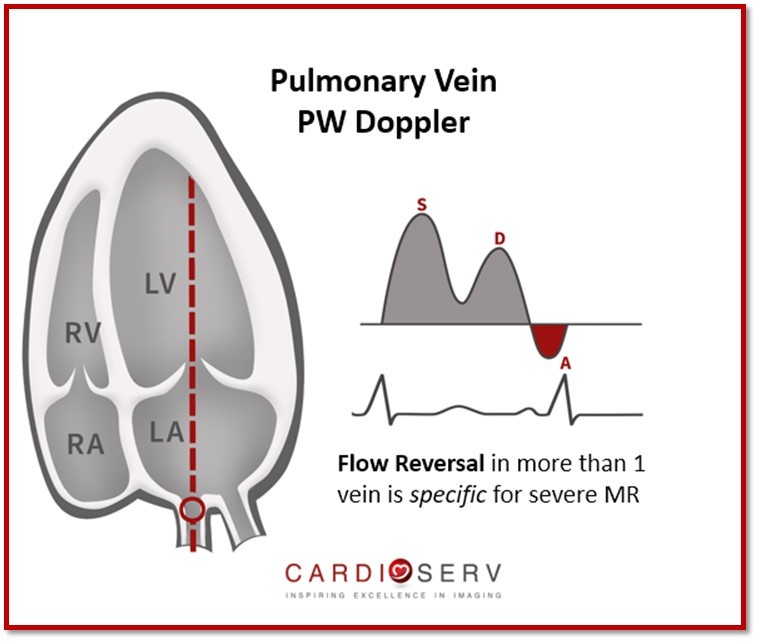
Pulse Wave (PW) Doppler of Pulmonary Veins
We can Doppler the pulmonary veins to evaluate for flow reversal and the hemodynamics due to MR.
- Apical 4 window
- Sample volume of Doppler 1 cm into pulmonary vein
- Do not Doppler a vein that regurgitation is dumping into; attempt more than one vein in this case
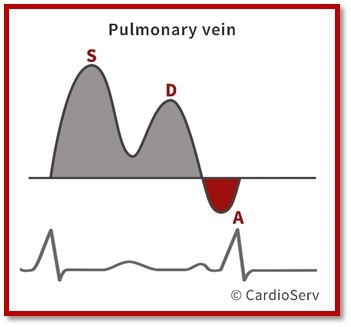
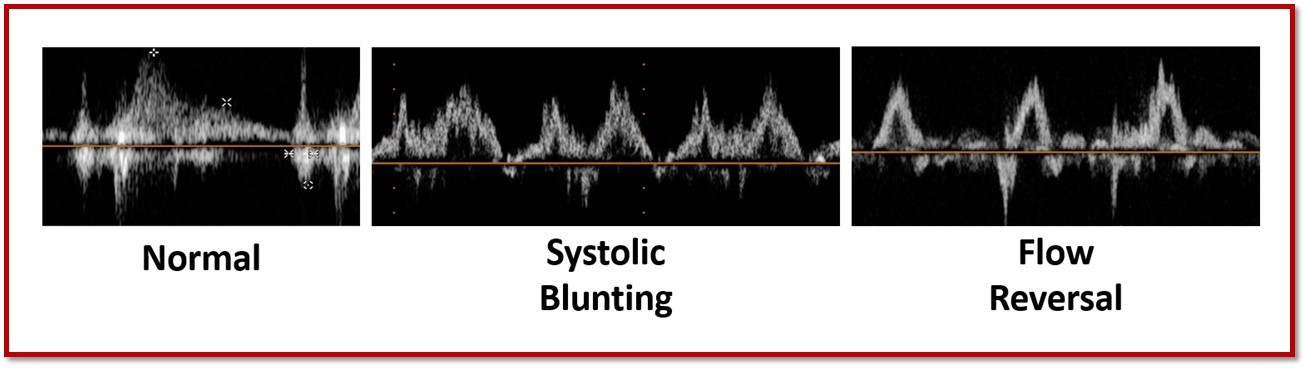
Components of pulmonary vein waveform:
- S Wave: systolic
- D Wave: diastolic
- A Wave: peak reversal flow
- Ar Duration: time of peak reversal flow (atrial contraction)
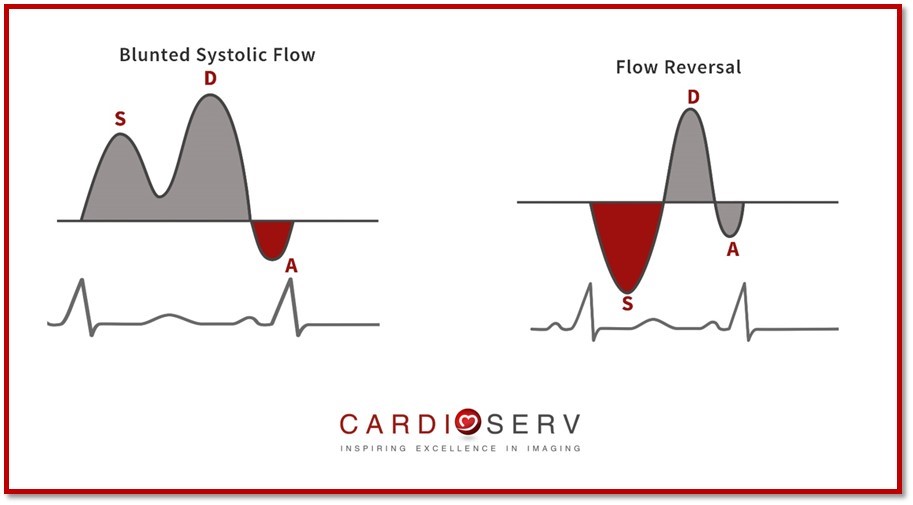
Flow reversal pattern is present, there is > 85% probability of severe MR.
Items to note in pulmonary vein Doppler:
- Systolic blunted flow does not automatically indicate moderate MR- could be the result of diastolic dysfunction.
- Normal flow pattern suggest low LAP & non-severe MR
- Less valuable in secondary MR due to unable to exclude diastolic dysfunction
Summary
Evaluating mitral regurgitation requires more than just a color Doppler jet — it demands a full hemodynamic perspective. By combining the three Doppler methods — CW Doppler of the MR jet, PW Doppler of the mitral inflow, and PW Doppler of the pulmonary veins — we can accurately assess MR severity and its physiologic impact.
Each Doppler view contributes unique insight:
- CW Doppler defines jet velocity and contour.
- Mitral inflow PW highlights diastolic changes.
- Pulmonary vein PW reveals atrial response and flow reversal.
When integrated with color Doppler and 2D findings, these parameters provide a reliable, comprehensive evaluation of MR.
Take the Guesswork Out of Mitral Valve Imaging
Mitral Valve Imaging in Echo – Visual Guide
Sharpen your MR assessment with this clear, image-rich guide to echo views, scallops, and probe positioning.
- ✔ Understand scallop anatomy in TTE & TEE with ease
- ✔ Avoid common pitfalls like foreshortened views
- ✔ Dozens of labeled diagrams for quick reference
- ✔ Practical checklists to streamline MR imaging
Ready to Go Even Deeper?
If you’re ready to move beyond these Doppler techniques for mitral regurgitation, our CME course, Mitral Regurgitation: Advanced Quantification, takes you step-by-step through all three quantitative methods of assessing MR severity — PISA, Stroke Volume, and Volumetric — using real case examples and guideline-based interpretation.
You’ll learn how to:
- Apply each method in challenging MR cases
- Recognize common measurement pitfalls
- Integrate findings to determine MR severity with confidence
Plus, you’ll earn 5 CME credits!
The course deep dives into MR quantification but teaches the material in a simple and easy way to make learning fun!

Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Zoghbi, W. A., MD, FASE, & Adams, D., RCS, RDCS, FASE. (2017). Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation. JASE, 30, 4th ser., 1-69. Retrieved June 12, 2017.