When “Fluid Around the Heart” Isn’t the Whole Story
Even though pericardial disease is a fairly common finding in echo, it also happens to be one of the most underrecognized and misinterpreted conditions in cardiac imaging.
As cardiac sonographers we often describe what we see: “a small effusion,” “a large circumferential effusion”, etc
But the real clinical question is:
👉 Is it just fluid surrounding the heart… or is it affecting cardiac function?
While we often think of the pericardium as a protective sac, it’s so much more than that. Under normal conditions, it moves and stretches with every heartbeat, quietly accommodating changes in volume and pressure.
But when it loses that flexibility, the pericardium can transmit pressure back to the heart or even restrict its ability to fill.
And that’s where the spectrum of pericardial disease begins. A continuum that ranges from simple effusion to hemodynamic tamponade and, in chronic or recurrent inflammation, to constriction. Understanding this progression changes the way we view the pericardium and how we interpret our echo findings.
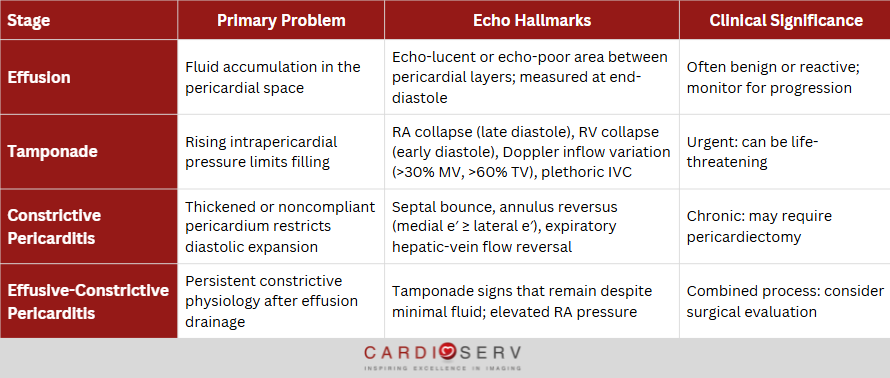
The Spectrum of Pericardial Disease at a Glance
Think of pericardial disease not as isolated conditions, but as a continuum of pressure and compliance.
Each stage represents a different point along that curve, from simple volume accumulation to fixed mechanical restriction.
Recognizing where your patient falls on this spectrum is what transforms observation into diagnosis.
Don’t stop at identifying an effusion. Always ask, “What’s the physiology?”That one question will lead you to the right side of the spectrum every time.
The “Pericardial Three-Step” Framework
Every pericardial study, no matter how simple or complex, should start with these three questions:
Is there fluid?
Is there increased pressure?
Is there restriction?
1. Is there fluid?
Measure it. Quantify it. Describe its location.
Report size of the effusion in millimeters at end-diastole, and specify whether it’s posterior, anterior, or circumferential.
A small effusion might not be clinically significant, but a moderate or large collection of fluid can tip into hemodynamic compromise depending on how fast it accumulates.
Size matters less than rate of accumulation. A small acute effusion can be far more dangerous than a large chronic one.
2. Is There Increased Pressure?
Look for the signs of rising intrapericardial pressure. How do you do this? Look for chamber collapse, Doppler inflow variation, or IVC plethora.
These findings tell you when the pericardium is no longer just storing fluid, but transmitting pressure back to the heart.
RA collapse in late diastole when RA pressure is lowest.
RV collapse in early diastole when RV pressure is lowest.
Doppler inflow variations:
Mitral valve (MV) inflow E-wave velocity variation > 30% between inspiration and expiration
Tricuspid valve (TV) inflow variation > 60%
Pressure defines tamponade, not the amount of fluid.
3. Is There Restriction?
Assess for loss of pericardial compliance, which is the point where diastolic filling becomes limited despite equalization of chamber pressures.
Look for:
Septal bounce or abrupt early-diastolic motion
Annulus reversus: Medial e′ ≥ lateral e′
Expiratory hepatic-vein diastolic flow reversal
When these features appear, you’ve moved from a pressure problem to a compliance problem, the hallmark of constrictive pericarditis.
CardioServ Takeaway
This three-step approach keeps your interpretation anchored in physiology.
By answering the three questions, “Is there fluid, pressure, or restriction?” you’ll never miss the transition from a benign effusion to clinically significant pericardial disease.
Echocardiography: The Cornerstone of Pericardial Evaluation
Echocardiography remains the first-line and most powerful imaging tool for evaluating pericardial disease. Not because it shows the anatomy best, but because it captures physiology in real time.
No other imaging modality can visualize real time chamber interaction, respiratory variation, or hemodynamic compromise as fast and as accurately as echocardiography.
CT and MRI can define pericardial thickness, calcification, or inflammation, but only echo reveals how those changes actually affect cardiac filling and output.
The Clinical Impact
Recognizing where a patient falls on the spectrum of pericardial disease isn’t just an academic exercise, it’s what guides management.
Each point along that continuum represents a different physiologic problem which requires a different clinical response.
A moderate effusion may only require follow-up and risk-based monitoring.
Tamponade demands immediate drainage and hemodynamic stabilization.
Constriction often calls for surgical pericardiectomy once the diagnosis is confirmed.
An effusive-constrictive process requires you to think beyond “fluid removal” and address the constrictive component beneath.
CardioServ Takeaway
Each diagnosis lies on the same path — the only difference is where you catch it.
The earlier you recognize the physiology, the more precisely you can intervene.