Last Updated on November 18, 2025 by Don Gerig, RDCS
For years, right heart echo has focused on diagnosis. The 2025 ASE guidelines push us further, using the same parameters not just to identify disease, but to predict outcomes.
This is Part 1 of our series breaking down the 2025 ASE Right Heart Guidelines. Today, we’ll highlight the big-picture shift from diagnosis to prognosis. In the coming weeks, we’ll dive into new cutoffs, severity ranges, and prognostic markers you can apply in your lab.
Historically, sonographers have been trained to capture RA size, RV function, TR velocity, and IVC dimensions as diagnostic clues.
- Was the RA or RV enlarged?
- Was TR velocity elevated?
- Was TAPSE abnormal?
- Did the IVC collapse?
The answer often stopped at “yes” or “no”. Diagnosis not prognosis.
The 2025 ASE Guidelines for the Echocardiographic Assessment of the Right Heart in Adults and Special Considerations in Pulmonary Hypertension flip that script. These parameters are no longer just boxes to check. They are prognostic markers that help predict hospitalization, survival, and response to therapy.
While the new guidelines cover the entire right heart, they give special weight to pulmonary hypertension, where the evidence for prognosis is strongest. This shift matters for every sonographer and cardiologist performing and interpreting echo.
Understanding Prognostic Right Heart Assessment: Structure, Function, and Hemodynamics
Traditional right heart assessment has often been binary: abnormal or not, high pressure or not. But that approach misses the spectrum of dysfunction we see every day. Two patients with the same elevated RVSP may have completely different outcomes.
The 2025 guidelines emphasize a three-pillar model: STRUCTURE – FUNCTION – HEMODYNAMICS.
This framework allows echocardiography to move beyond diagnosis to risk stratification, therapy tracking, and anticipating disease progression.
- Structure: RA and RV size, PA diameter
- Function: TAPSE, S′, FAC, strain, 3D RVEF
- Hemodynamics: TR velocity, RA pressure/IVC, RV–PA coupling
When these parameters are put together, echo provides more than a snapshot. It tells a story—not just what the heart looks like now, but where it may be headed.
For example, every 1 cm² increase in RA area correlates with higher morbidity and mortality in pulmonary hypertension patients. That’s the level of prognostic power we’re talking about!
The Evolution of Right Heart Assessment in Echocardiography
Right heart assessment has evolved significantly over the past 15 years. Here’s a snapshot:
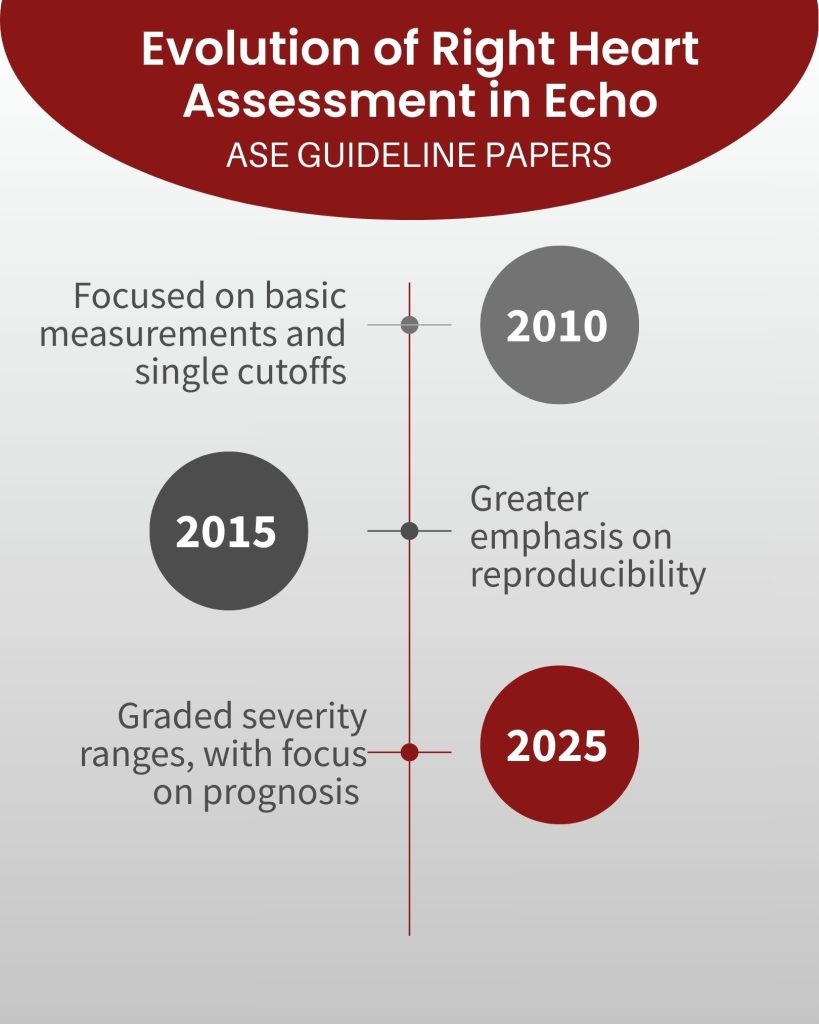
2010 ASE Right Heart Guidelines:
- Focused on basic measurements and single cutoffs.
- Example: TR velocity >2.8 m/s flagged pulmonary hypertension.
- Helpful for diagnosis, but mostly binary.
2015 ASE Chamber Quantification Guidelines:
- Expanded measurement standards, especially for RV and RA.
- Greater emphasis on reproducibility.
- Outcomes sometimes mentioned, but framework remained focused on structure.
2025 ASE Right Heart & Pulmonary Hypertension Guidelines:
A paradigm shift: The 2025 guidelines shift right heart echo from finding disease to forecasting outcomes
- Graded RV function parameters (TAPSE, S′, FAC, 3D RVEF, strain)
- Indexed RA/RV volumes with severity ranges
- Graded TR velocity
- RV–PA coupling (TAPSE/PASP ratio) and RV strain as explicit prognostic markers
- Probability models (low, intermediate, high) replacing single cutoffs
Looking Ahead
This is just the beginning. Next week, we’ll dive into the specific changes in the 2025 ASE guidelines—including new cutoffs, severity ranges, and prognostic markers—so you can start applying them in your echo lab with confidence.
Related Articles

Don Gerig, RDCS, Medical Education Manager
Connect on LinkedIn