
Last Updated on November 19, 2025 by Judith Buckland, MBA, RDCS, FASE
The right ventricle (RV) is now fully recognized as a key driver of outcomes across multiple disease states — including pulmonary hypertension (PH), valvular heart disease, congenital heart disease, and heart failure.
For sonographers and cardiologists, the challenge lies not only in imaging the RV but in understanding how it responds and adapts to pressure overload. As pulmonary pressures rise, the RV can adapt successfully for a time… until those mechanisms fail.
In this article, we’ll explain how to differentiate adaptive vs maladaptive right-ventricular remodeling in pulmonary hypertension using echocardiography, highlighting key imaging features, physiologic differences, and what each pattern means clinically.
Understanding Right Ventricular Remodeling in PH
First we need to understand that the right heart remodeling in pulmonary hypertension follows a continuum rather than a single event.
- Early Phase: The RV adapts to increased afterload through hypertrophy and augmented contractility.
- Progressive Phase: As the disease advances, the RV can no longer sustain this response. Contractility becomes insufficient, leading to dilation, rising filling pressures, and eventual right heart failure.
Next we need to recognize this transition from adaptive to maladaptive remodeling — and the corresponding shift from coupling to uncoupling — is critical for prognosis, risk stratification, and therapeutic timing.
🟢 Adaptive Right Ventricular Remodeling
Defining Adaptive Remodeling
Initially, early compensatory response of the RV to increased afterload. To overcome the increase in afterload the initial adaptive response to PH is the RV’s effort to increase contractility. The increased contractility results in an increase in tissue thickness and mass.
In this stage, the RV increases its contractility to preserve forward flow. To support this, it undergoes concentric hypertrophy, thickening the wall to normalize wall stress and maintain stroke volume.
Echocardiographic Features of Adaptive Remodeling
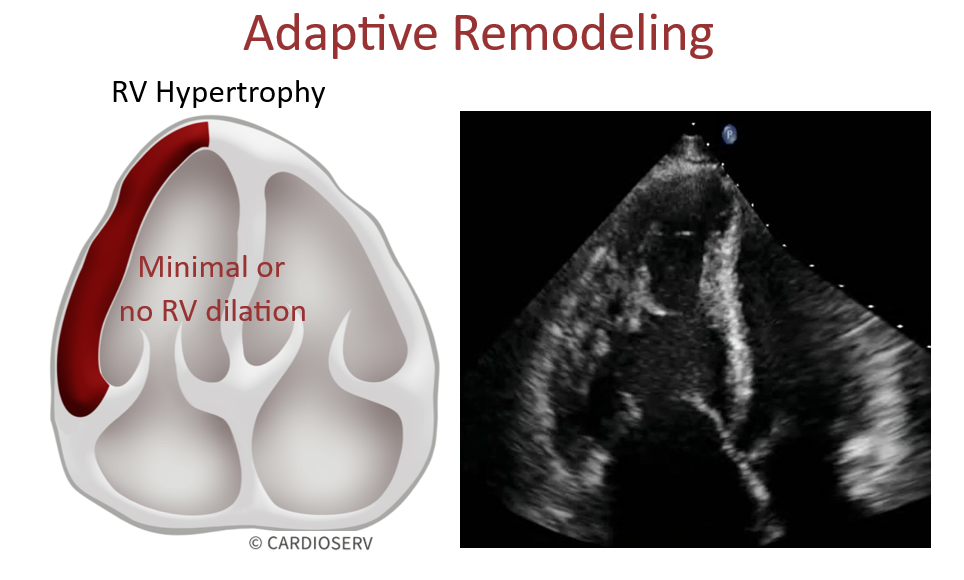
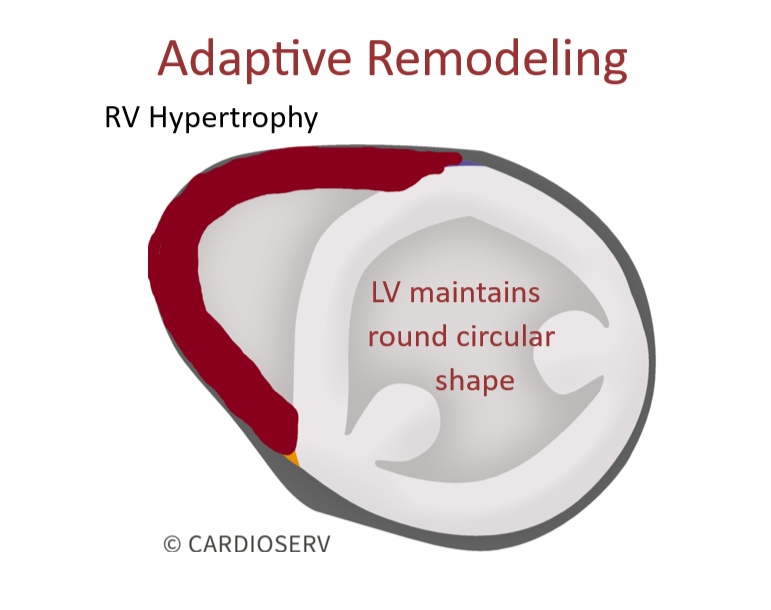
- Concentric RV hypertrophy (increased wall thickness, normal cavity size)
- Preserved RV systolic function (normal TAPSE, S′, FAC, strain)
- Minimal or no RV dilation
- Normal interventricular septal curvature (round LV)
Clinical Implications of Adaptive Remodeling
- The RV successfully maintains cardiac output despite elevated afterload.
- Patients are often asymptomatic or mildly symptomatic.
- This corresponds to a coupled RV–PA state.
🔴 Maladaptive Right Ventricular Remodeling
At this stage, the RV reaches the limits of its adaptive capacity. Next, the contractile reserve is exhausted and the systolic function declines. RV dilation replaces earlier hypertrophy.
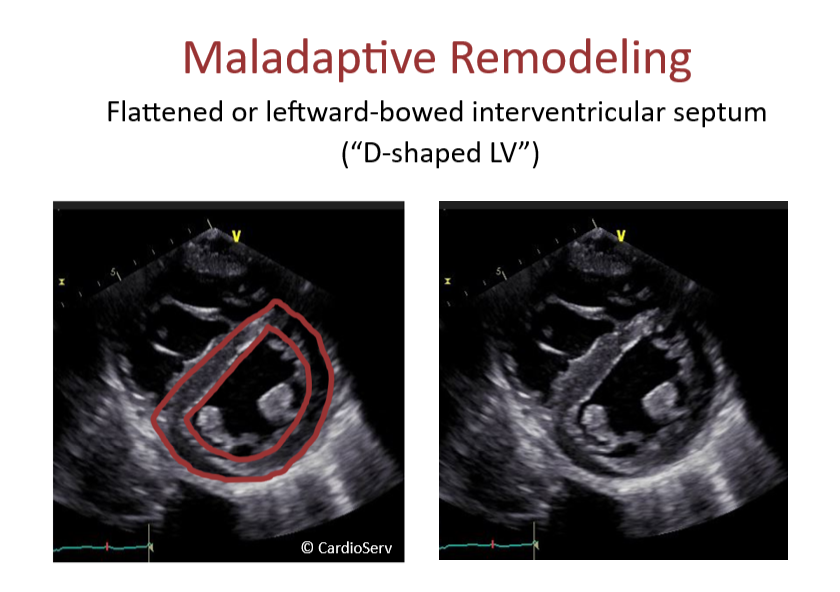
Echocardiographic Features of Maladaptive Remodeling
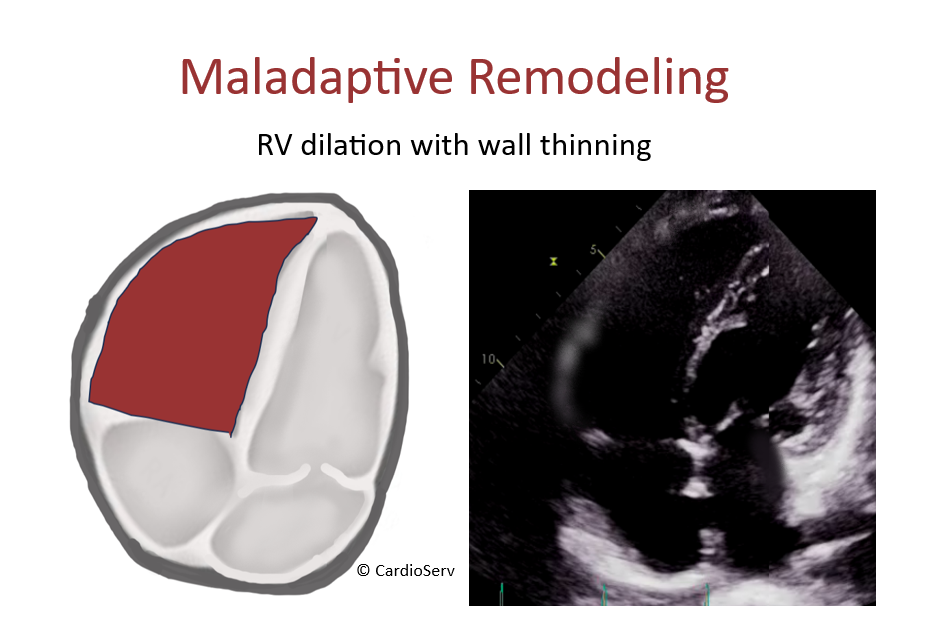
- RV dilation with thinning of the wall
- Reduced systolic function:
- TAPSE ↓ (<17 mm)
- S′ ↓ (<9.5 cm/s)
- FAC ↓ (<35%)
- RV longitudinal strain less negative than –20%
- Flattened or leftward-bowed interventricular septum (“D-shaped LV”)
- Right atrial enlargement, annular dilation, and functional TR
Clinical Implications of Maladaptive Remodeling
- Declining stroke volume and cardiac output
- Rising right atrial pressure and systemic congestion
- Associated with onset of right heart failure, rising symptoms, and poor prognosis.
- RV-PA uncoupling (contractility no longer matched to afterload)
Comparing Adaptive and Maladaptive Patterns
| Pattern | Echo Findings | Clinical Meaning |
|---|---|---|
| Adaptive (compensated) | RV thickening, concentric remodeling, preserved function, minimal dilation | Early stage; RV maintains cardiac output despite elevated afterload. |
| Maladaptive (decompensated) | RV dilation, wall thinning, septal flattening, RA enlargement, reduced function | Advanced stage; RV–PA uncoupling, rising filling pressures, poor prognosis. |
Conclusion
Putting the pieces together we understand that right-ventricular remodeling in pulmonary hypertension is a story of adaptation versus exhaustion.
- In its early, adaptive phase, the RV responds intelligently—thickening its wall and boosting contractility to preserve forward flow and protect the left ventricle.
- Over time, persistent pressure overload overwhelms this system, leading to maladaptive changes marked by dilation, declining function, and rising right-sided pressures.
Recognizing where your patient lies on this spectrum is critical: it allows you to anticipate decompensation, adjust therapy, and monitor response.
In the next post, we’ll explore how this structural story translates into efficiency—through the concept of RV–pulmonary artery coupling.
Related Articles and Resources
- Pulmonary Hypertension Case Study Presentation
- Understanding Pulmonary Hypertension in Echo
- Mastering TAPSE in 2025: Graded Severity, Pitfalls, and Best Practices
- 2025 ASE Right Heart Guidelines

Judith Buckland, MBA, RDCS, FASE
Connect on LinkedIn




