Last Updated on November 18, 2025 by Don Gerig, RDCS
The 2025 ASE Right Heart Guidelines redefine how we evaluate the right ventricle by shifting the focus from diagnosis to prognosis. The new framework integrates structure, function, and hemodynamics to give a complete picture of right-heart performance and patient outcome.
Within this model, however, TAPSE (Tricuspid Annular Plane Systolic Excursion) remains a cornerstone of RV systolic function because it’s simple, reproducible, and available in every echo lab. Yet, its role has evolved.
Rather than relying on a single cutoff, the 2025 guidelines introduce graded severity ranges and stress combining TAPSE with other RV parameters for a more accurate, prognostically meaningful assessment.
In this article, we’ll show how to measure TAPSE correctly, apply the new grading, recognize common pitfalls, and interpret results within the broader right-heart framework.
What Is TAPSE?
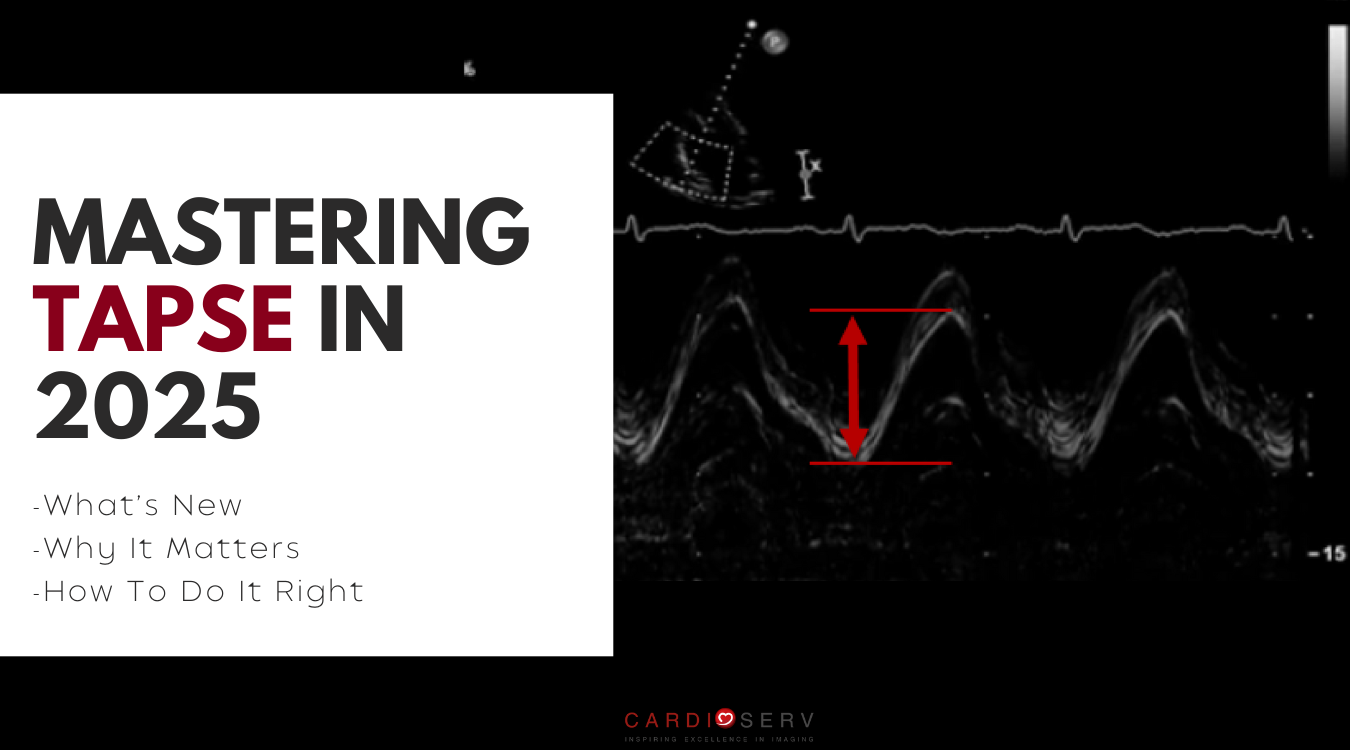
TAPSE (Tricuspid Annular Plane Systolic Excursion) measures how far the lateral tricuspid annulus moves toward the apex during systole. This motion reflects the RV’s longitudinal shortening, which is the dominant contributor to right ventricular systolic function.
On echo, you’ll see it as the vertical motion of the tricuspid annulus on M-mode. Because it’s simple, reproducible, and available in all echo labs, TAPSE has become one of the most widely used parameters of RV systolic performance.
What’s Changed
Simple, fast, and reproducible — TAPSE has earned its place as the workhorse of RV systolic function.
For years, TAPSE was defined by one number: <1.7 cm was abnormal. The 2025 guidelines changed that by introducing graded severity ranges, giving sonographers and physicians a more meaningful way to describe and communicate RV function.
Instead of just “normal” or “abnormal,” we can now report TAPSE as normal, mild, moderate, or severely reduced.
TAPSE Graded Severity Ranges
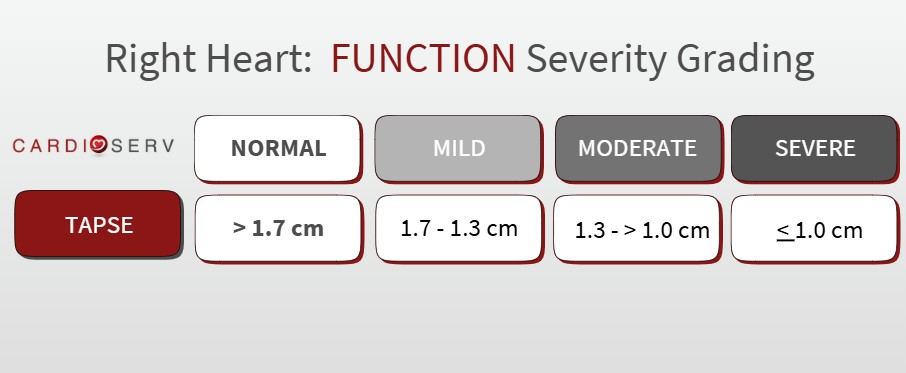
*Note: TAPSE 1.3 cm is graded as both mild and moderate per ASE Guidelines
Why It Matters
- Distinguishes mild, moderate, and severe RV dysfunction, which helps with prognosis and clinical decision-making.
- Improves consistency across labs by standardizing how TAPSE results are reported.
- Brings TAPSE in line with how other RV function parameters (S′, FAC, RV strain) are graded, creating a more cohesive approach to RV assessment.
- Together, these updates strengthen TAPSE’s role within the 2025 ASE framework from a quick measurement to a reliable prognostic tool.
Why TAPSE Should Never Stand Alone
The 2025 ASE guidelines make it clear: TAPSE is valuable, but it’s not enough on its own. It must be interpreted within the full right-heart framework — integrating structure, function, and hemodynamics to avoid misclassification and improve prognostic accuracy.
On its own, TAPSE measures motion, not load. That means it can look normal even when RV contractility is impaired, or appear reduced when loading conditions change. To strengthen interpretation, TAPSE should be considered alongside other indices such as S′, FAC, 3D RVEF, and RV–PA coupling (TAPSE/PASP ratio).
While TAPSE is simple and reproducible, it does have its limitations. Below are common situations where TAPSE can be misleading:
- Underestimation of RV function: Seen with suboptimal image quality, poor M-mode alignment, constrictive pericarditis (restricted motion despite preserved function), catheters or pacemaker leads, and post-cardiac surgery changes.
- Overestimation of RV function: Occurs with severe functional TR causing annular distortion, abnormal loading conditions, or right-heart maladaptation.
When interpreted as part of a multiparametric approach, TAPSE remains one of the most dependable tools for assessing RV systolic performance.
How to Perform TAPSE Measurement
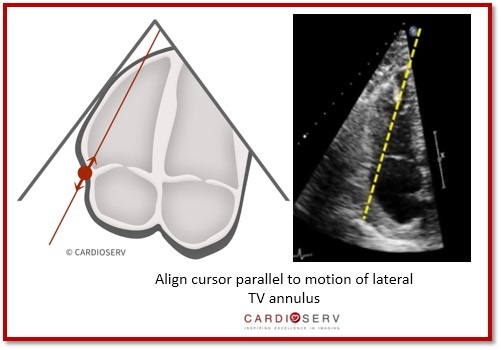
TAPSE is measured using M-mode through the lateral tricuspid annulus in the RV-focused apical four-chamber view. The distance between the end-diastolic and end-systolic positions of the annulus represents RV longitudinal shortening.
- Use the RV-focused apical 4-chamber view.
- Place the M-mode cursor through the lateral tricuspid annulus, aligned with the direction of annular motion.
- Ensure the annulus is moving toward the apex during systole.
- Adjust gain settings to reduce noise and clearly visualize annular motion.
- Record at a medium-to-fast sweep speed for accuracy.
- Identify maximum systolic and diastolic excursion of annulus motion
- Measure the excursion vertically, leading-edge to leading-edge.
💡 Pro Tip: Even minor misalignment of the M-mode cursor can lead to significant underestimation. So, be sure to check your cursor angle before freezing and measuring.
Final Thoughts and Next Steps
The 2025 ASE guidelines move TAPSE beyond a single cutoff to graded severity, making it a stronger tool for both sonographers and physicians. For labs, this update supports consistency. For patients, it means earlier recognition of RV dysfunction and clearer communication of risk.
Go Deeper!
Want to master TAPSE in practice? Our updated CME course — Right Heart Quantification: TAPSE and S′ Wave — walks through everything you need to know. You’ll learn step-by-step how to perform TAPSE, avoid common measurement errors, and apply TAPSE and S′ as part of a comprehensive evaluation of RV function. Plus, you’ll earn 1 CME credit!
(Earn 1 CME credit and master TAPSE)
Ready to Go Beyond TAPSE?
For a complete roadmap to right-heart evaluation, explore the All Right Heart Quantification Modules Bundle You’ll cover every RV parameter — with step-by-step guidance, clinical integration, and 5.0 CME credits.
All RV parameters • Step-by-step guidance • Clinical integration
References
Mukherjee M, Rudski LG, Addetia K, et al. Guidelines for the echocardiographic assessment of the right heart in adults and special considerations in pulmonary hypertension: Recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr. 2025;38(3):141-186. doi:10.1016/j.echo.2025.01.006
Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39.e14. DOI:10.1016/j.echo.2014.10.003