Last Updated on October 16, 2025 by Don Gerig, RDCS
Evaluating the aortic valve is a routine part of an echocardiogram. There are many methods we use to determine the structure and function of the valve, including 2D, color Doppler and a combination of pulsed & continuous-wave Doppler.
Short examination times are far too common of a challenge, and moving too fast can lead to small technical errors that can lead to large clinical consequences.
The good news? Most errors are avoidable.
In this article, we’ll review four of the most common aortic valve Doppler measurement mistakes we make, and how to avoid them. This way you can be confident you’re reporting accurate data which leads to better interpretation and better patient outcomes.
4 Common Doppler Errors in Aortic Valve Measurements
1. Not Parallel To Flow
Not aligning your Doppler beam parallel to blood flow is one of the most common aortic valve Doppler errors that leads to the underestimation of peak velocity and ultimately, misclassification of the severity of aortic stenosis.
Let’s go back to the basics of ultrasound physics:
- Velocity, frequency, and angle all determine the frequency shift of sound waves within moving blood.
- The angle between the ultrasound beam and the direction of flow should be as close to zero degrees as possible, meaning the Doppler beam is parallel to blood flow.
- Any deviation from zero causes an underestimation of the true velocity, because the Doppler equation measures only the component of motion that aligns with the beam.
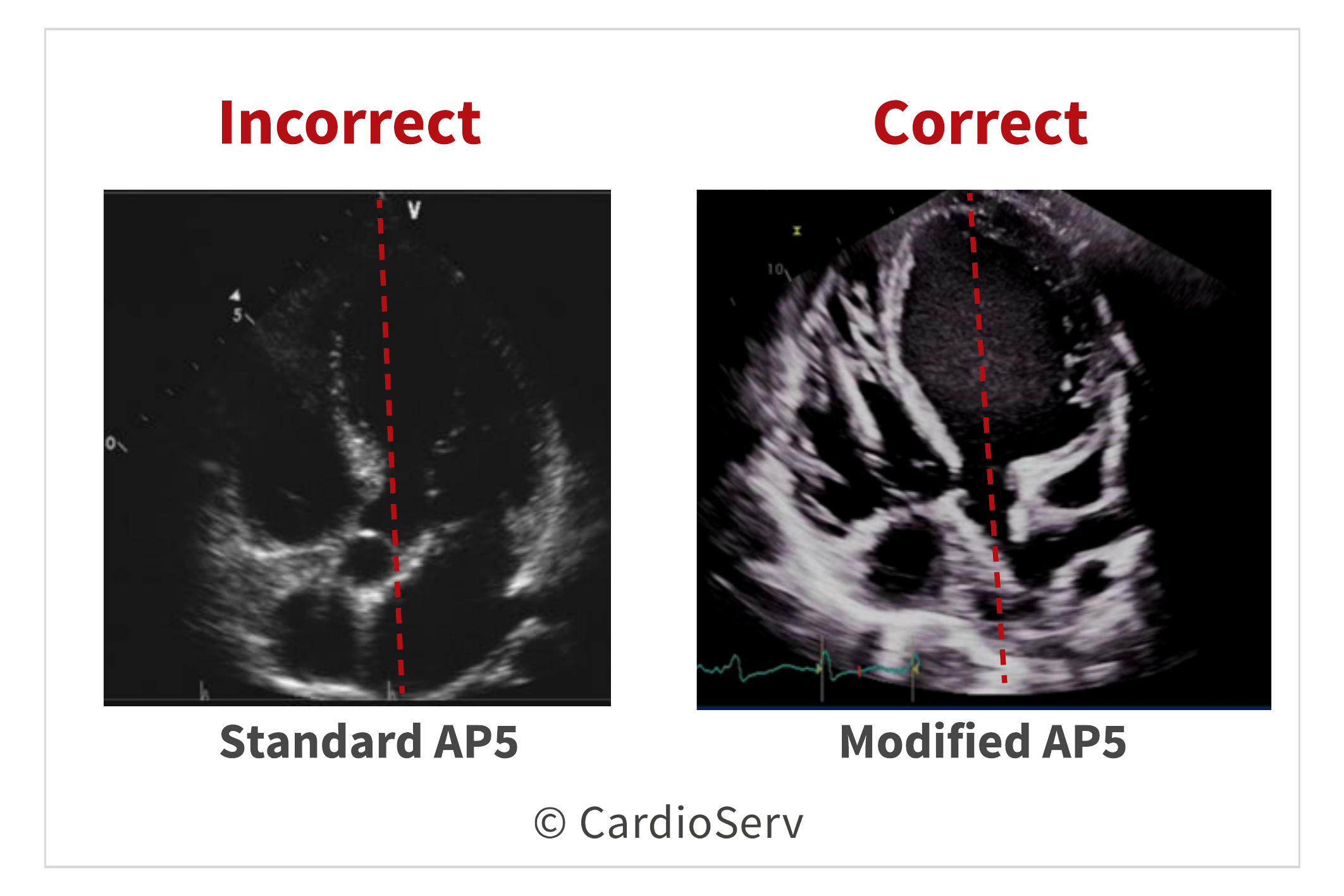
Scanning Tips
- Move the transducer more laterally on the patient’s chest to achieve better Doppler alignment.
- Ask the patient to lean back slightly to optimize the angle.
- Avoid using angle correction: it can introduce additional error and is not recommended for spectral Doppler of the aortic valve.
2. Measuring Artifact
Including artifact in your Doppler tracings is another common echo aortic valve measurement mistake that leads to inaccurate peak velocity and gradient calculation.
At the peak of the aortic valve CW Doppler waveform, you may notice fine, wispy linear signals that extend above the true envelope. These represent noise and artifact, not real blood flow, and should never be included in your velocity measurement.
When artifacts are traced, the peak velocity and associated pressure gradients become artificially elevated, leading to an overestimation in aortic stenosis severity.
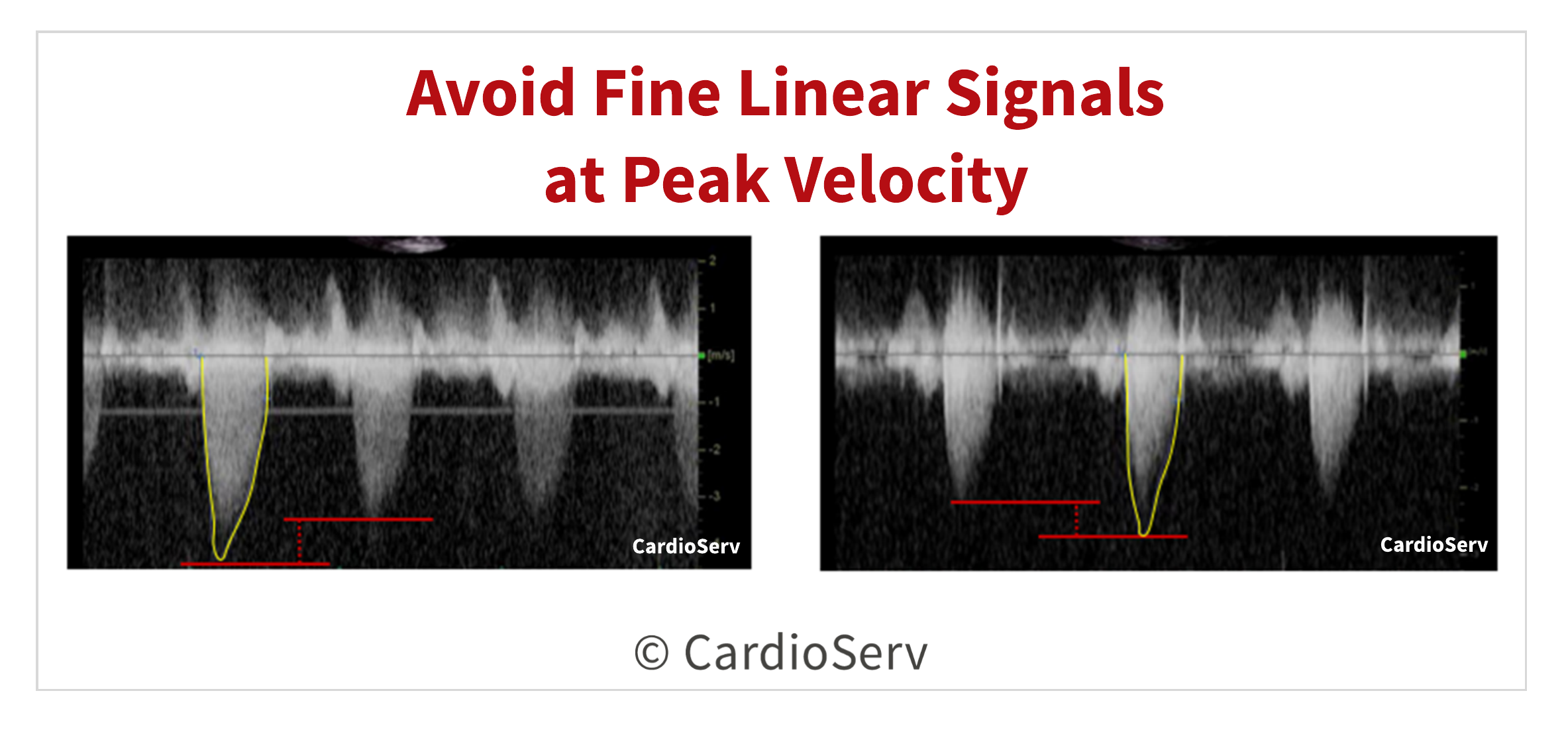
Scanning Tips
- Lower the Doppler gain until the artifact disappears while maintaining a clear spectral envelope.
- Reduce the Doppler scale to improve waveform resolution for accurate tracing.
- Never trace fine linear signals beyond the dense spectral display. These signals represent artifact, not flow.
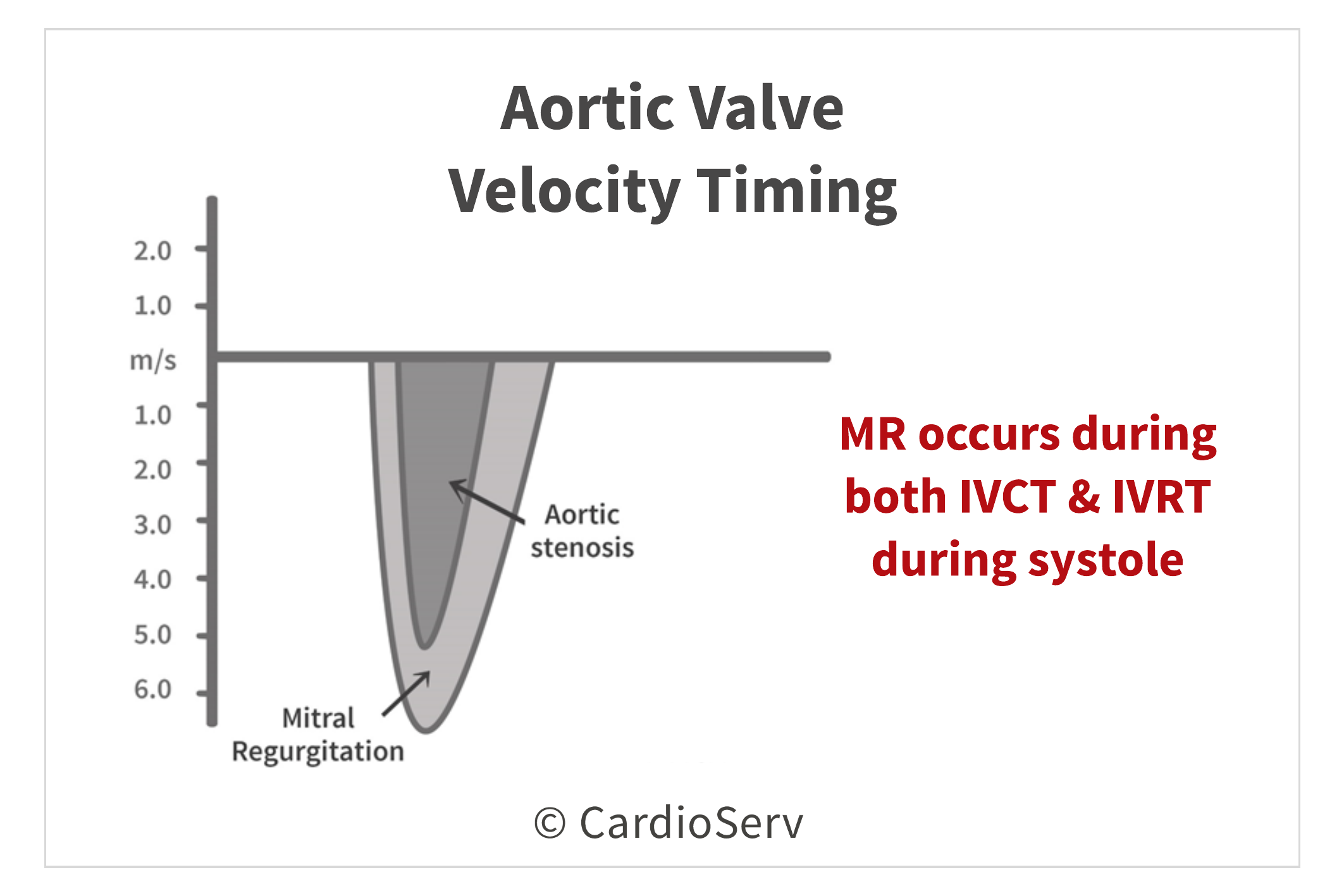
3. Measuring the Wrong Velocity Tracing
Mistaking mitral regurgitation (MR) velocity for aortic valve (AV) velocity is one of the easiest aortic valve Doppler errors to make, especially when both signals appear within systole. This mistake can dramatically overestimate the true aortic velocity and lead to a false diagnosis of severe aortic stenosis.
To avoid this common echo aortic valve measurement mistake, focus on timing and valve events.
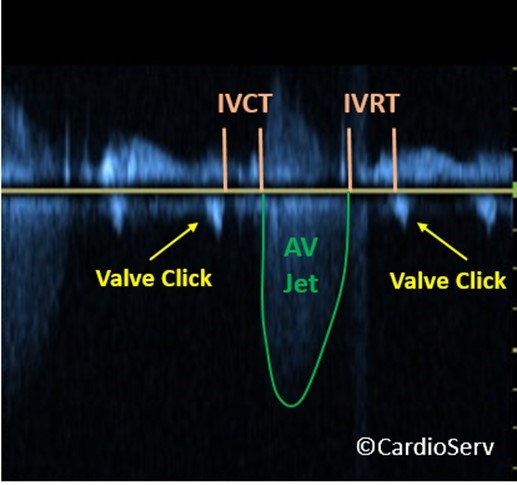
- MR velocity appears earlier in systole, extending through both the isovolumic contraction (IVCT) and isovolumic relaxation (IVRT) phases — times when both valves are closed.
- Aortic valve velocity, by contrast, begins after IVCT (once the valve opens) and ends before IVRT (when it closes).
By carefully correlating the timing of the Doppler envelope with the EKG and valve click markers, you can easily distinguish between the two.
Scanning Tips
- Identify valve clicks on the Doppler tracing to confirm opening and closing points.
- Correlate with the EKG to pinpoint IVCT and IVRT timing accurately.
- Do not trace early systolic MR signals — they occur before true aortic ejection.
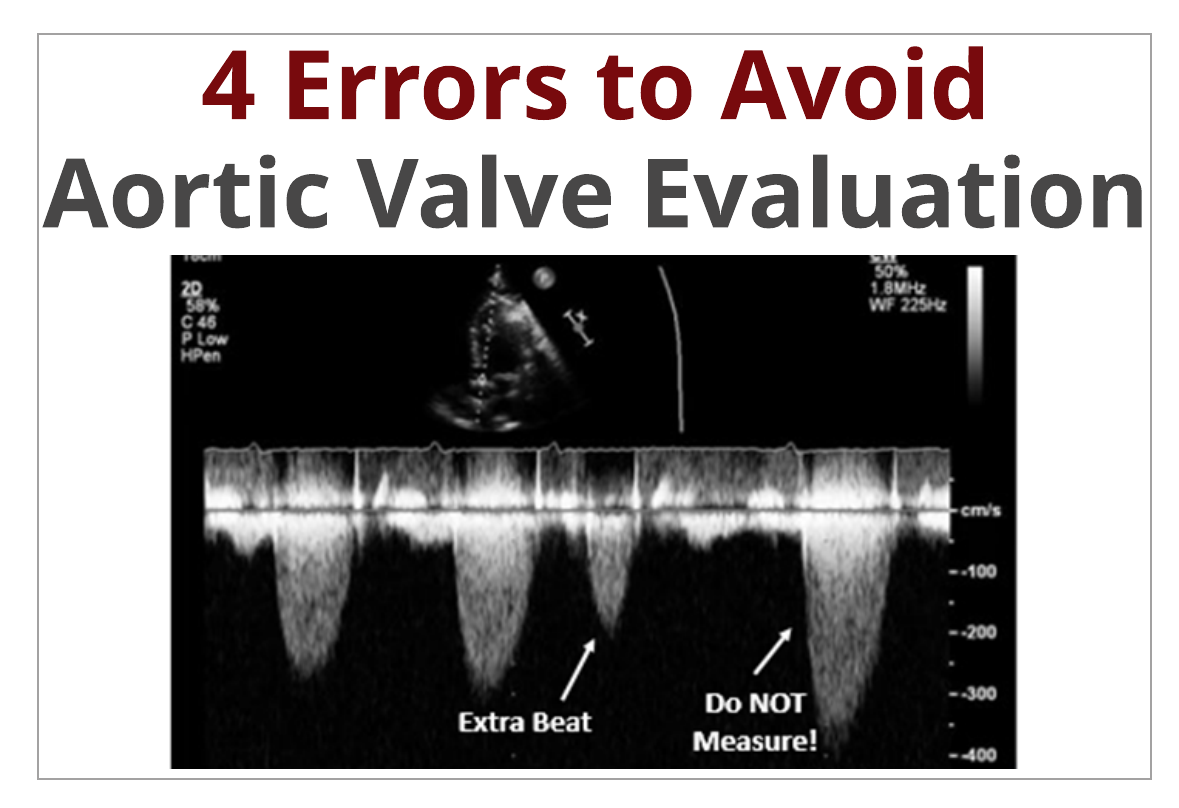
4. Measuring Post-Extrasystolic Beats
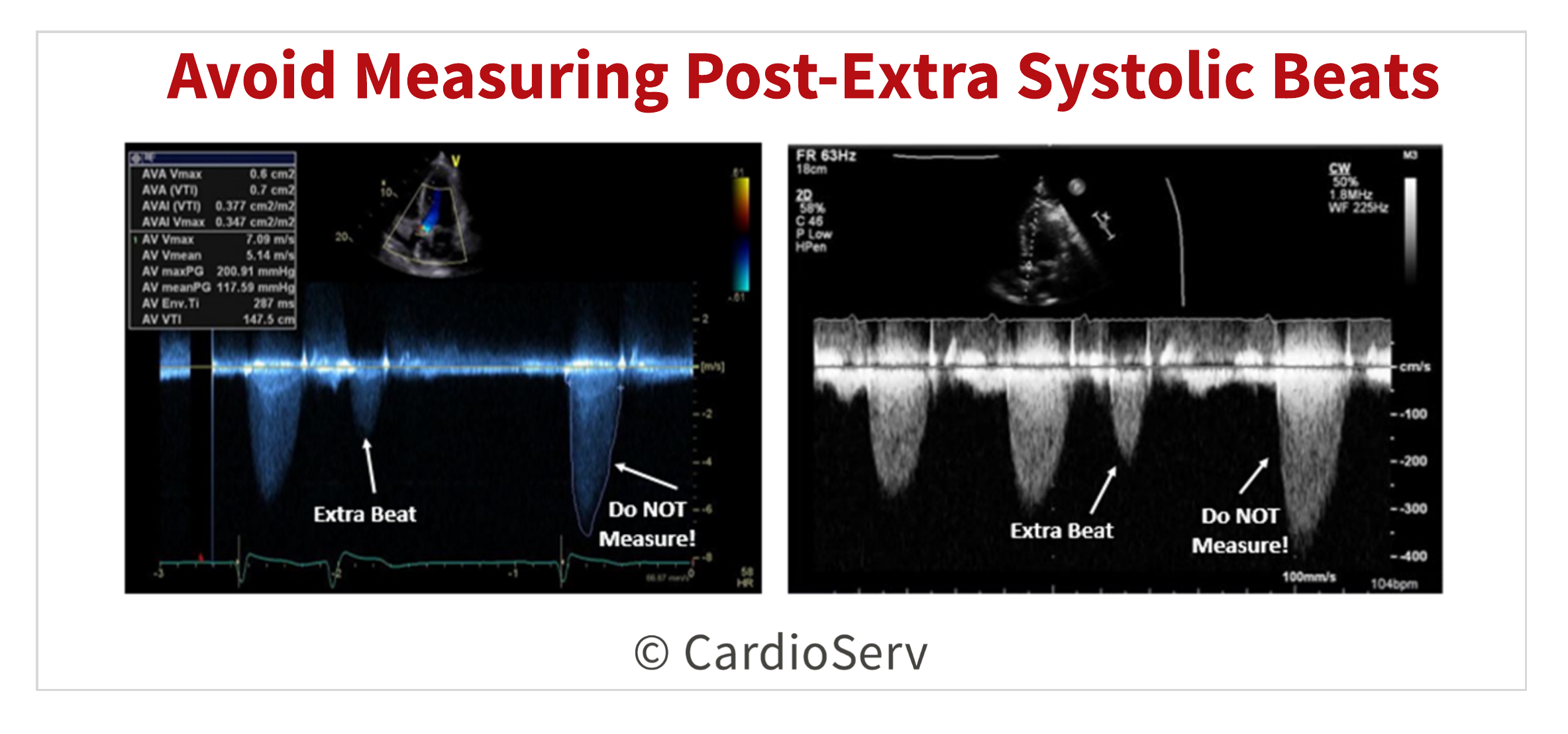
It’s not uncommon for patients to have premature ventricular contractions (PVCs) during an echo study. While we can’t prevent them, we can, and must, avoid measuring them.
Both the PVC beat and the post-extrasystolic beat (the beat immediately following a PVC) should never be used when measuring aortic valve Doppler velocity.
Here’s why:
After a PVC, the compensatory pause allows for increased ventricular filling and contractility, leading to higher stroke volume and artificially elevated velocities. If these beats are traced, they’ll overestimate the true aortic valve gradient, potentially exaggerating the severity of aortic stenosis.
Scanning Tips
- Let the Doppler signal run for several seconds to capture multiple beats for comparison.
- Only measure beats that are consistent in velocity and contour.
- In atrial fibrillation, measure and average 5–6 beats for both aortic valve (AV) and LVOT velocities.
Final Thoughts and Next Steps
When evaluating the peak aortic valve CW Doppler velocities, be sure to avoid these 4 common errors:
- Doppler Angle Not Parallel to Flow
- Measuring Fine Linear Artifact at Peak Velocity
- Measuring MR Velocity for Peak AV Velocity
- Measuring Extra-Post Systolic Beat Velocities
Go Deeper!
Every echo lab sees these aortic valve Doppler errors — the best ones know how to catch them. Take the next step in refining your Doppler technique with our CME course: 4 Errors to Avoid Measuring Aortic Valve Velocity
Learn to recognize each error, apply the correct scanning adjustments, and earn 0.25 CME credit while improving your diagnostic accuracy.

Andrea Fields MHA, RDCS
Stay Connected: LinkedIn, Facebook, Twitter, Instagram
References:
Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39.e14. DOI:10.1016/j.echo.2014.10.003




