
Last Updated on January 30, 2024 by Hannes van der Merwe
This week starts off our diastolic function blog series with our guest blog writer, Michael Owen! We introduced our followers to him last week- if you missed it, you can find it here! Our goal for this blog is to have a basic understanding of the normal ejection fraction (EF) algorithm for evaluating diastolic function!
Guest Writer: Michael Owen
RULE OUT PATHOLOGY FIRST
The 2016 diastology guidelines from the American Society of Echocardiography (ASE) now place heavier emphasis on clinical data as well as correlation with other modalities. At first glance, the guidelines undoubtedly seem quite overwhelming. However, when you really dissect the information, you might notice there are just a lot of “if-then” statements. There are many “if-thens” that even this attempt of simplification may seem daunting. I am going to remove the fluff and present you with the essentials!
The ASE provides two flow charts from the newly released guidelines. While these flow charts are easy to print out and use for the majority of patients, they are not accurate for special population patients. While assessing the patient, it is important to pay attention to pathology present on the left side of the heart. Specifically, you should look for any of the following because they will change the way you assess diastolic function:
- Atrial Fibrillation
- Hypertrophic Cardiomyopathy
- Restrictive Cardiomyopathy
- Sinus Tachycardia
- Moderate to Severe Mitral Regurgitation
- Mitral Stenosis
- Severe Aortic Insufficiency
- Heart Transplant Patients
- Cardiac causes of Pulmonary Hypertension
- Bundle Branch Block
We will cover how to evaluate diastolic function in all of these abnormalities, but first let’s focus on the common cases!
COMMON APPROACHES FOR ASSESSING DIASTOLIC FUNCTION
If you have successfully cleared the list above, you can simply follow the two flow charts outlined by ASE! When doing so, be careful to read the fine print underneath- you may find some nice surprises. To make things easier, I will dissect the two flow charts. The following two methods will be used for the majority of your patients.
ALGORITHM 1: NORMAL EJECTION FRACTION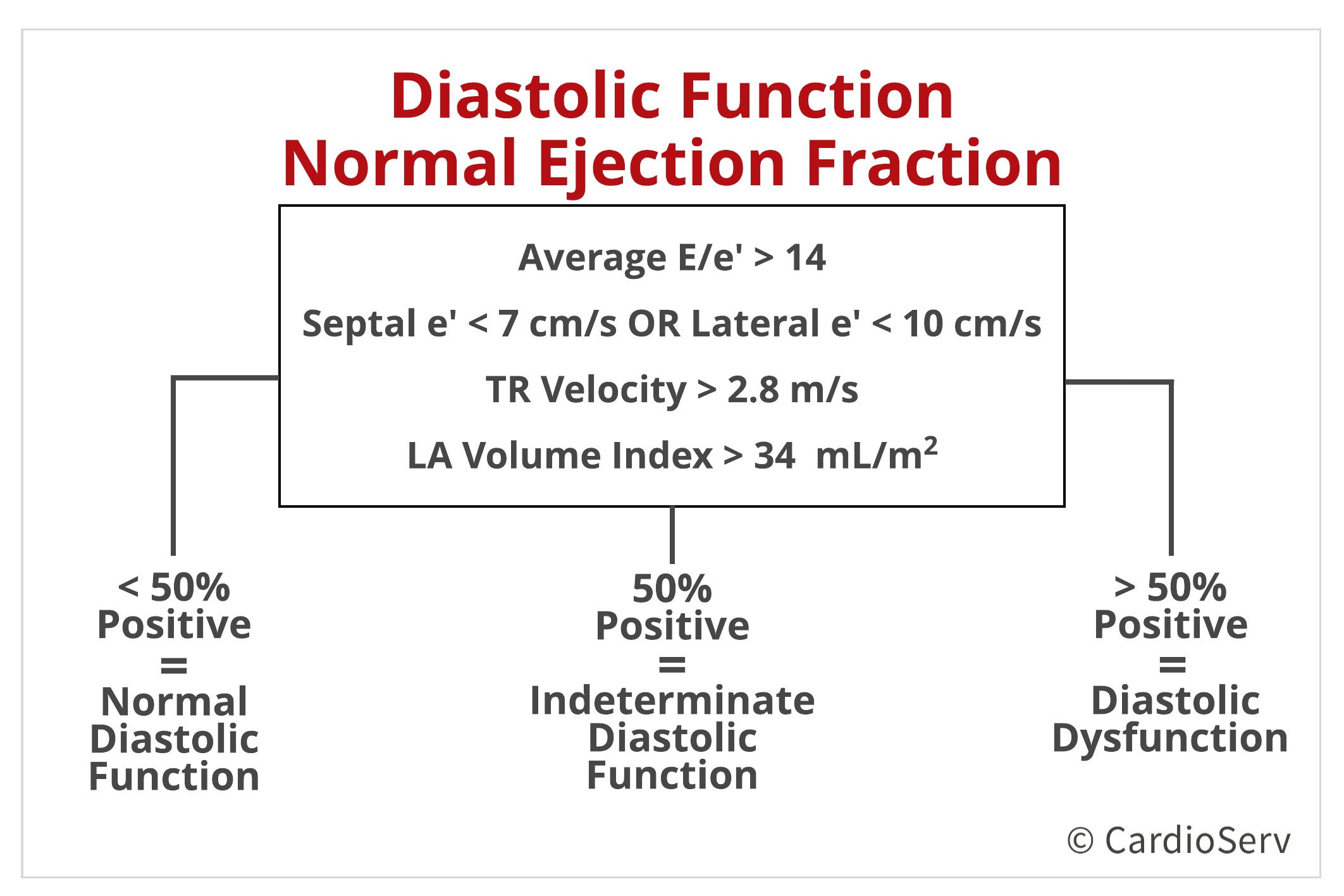
This chart regards patients with a normal ejection fraction and no myocardial disease. Notice the lack of emphasis on the mitral E/A ratio. Instead, you are focusing on the following parameters:
- Average E/e’
- Septal and Lateral e’ Velocities
- Tricuspid Regurgitation (TR) Velocity
- Left Atrial (LA) Volume Index
CUT-OFF VALUES
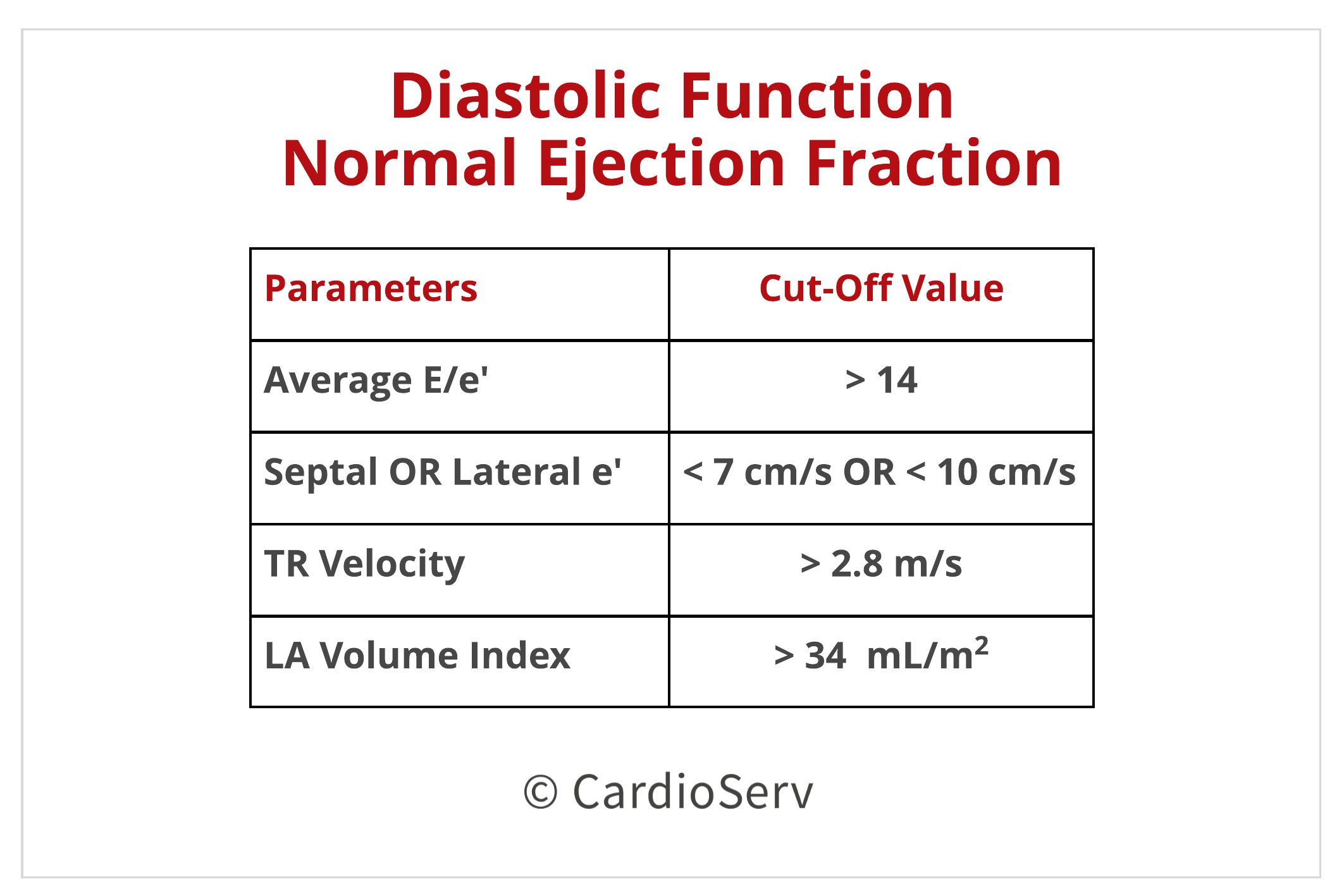
Simply compare your findings to ASE’s recommended cutoff values and see how many positives and negatives you come up with. Below are the cutoff ranges:
DETERMINE DIASTOLIC FUNCTION FINDINGS
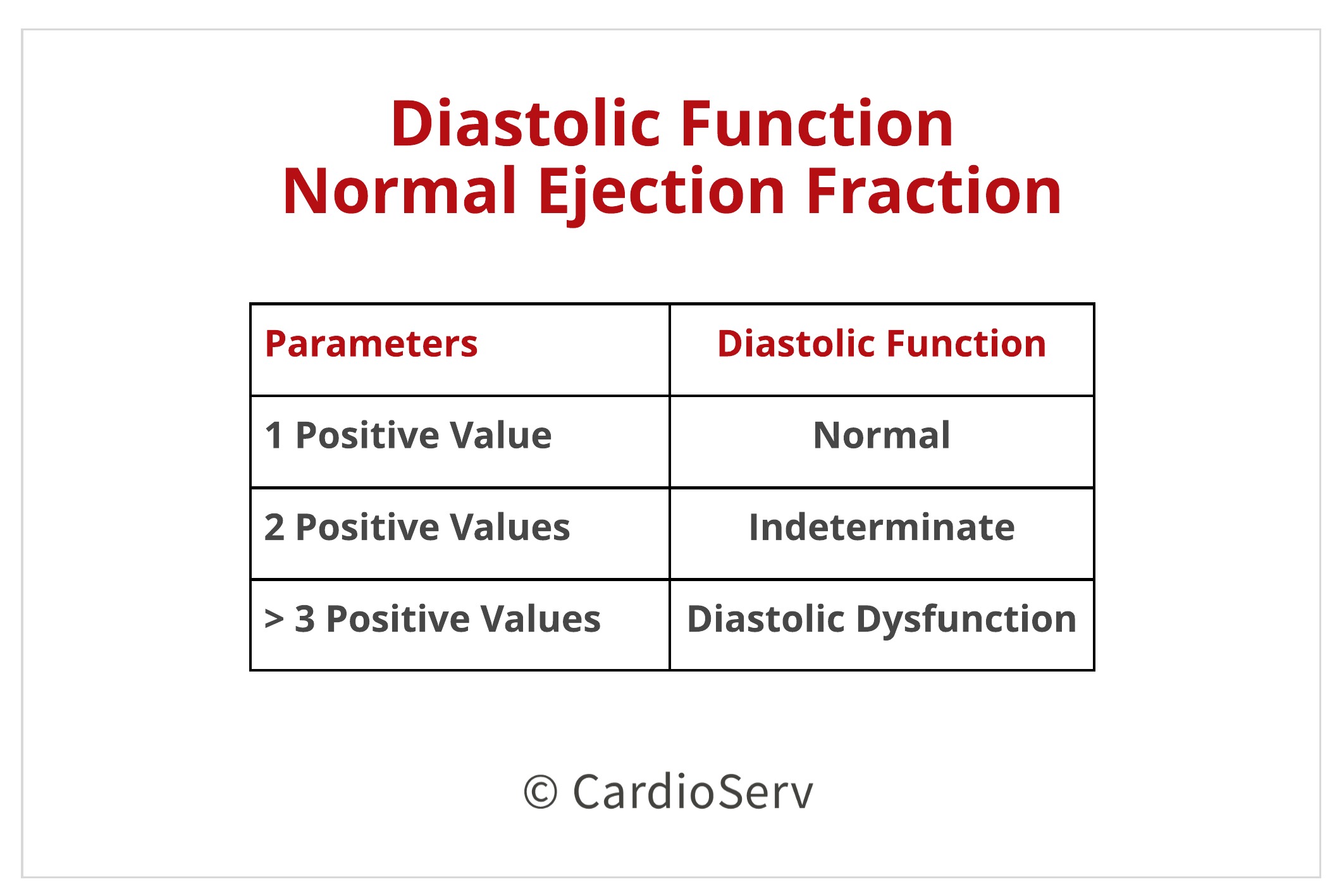
To determine if diastolic dysfunction is present, simply follow these guidelines:
- If only one of your values are positive, you have Normal Diastolic Function.
- If two of your values are positive, you have Indeterminate Diastolic Function.
- If three or more of your values are positive, you simply have Diastolic Dysfunction. (Note: The grade of dysfunction at this point as not been outlined by the ASE)
INDETERMINATE?!
I want to point out that, if you have arrived in the “Indeterminate Diastolic Function” category, there are other suggestive findings that indicate dysfunction. These include:
- Pulmonary venous AR duration exceeding Mitral A-wave duration by 30msec
- L-wave > 20 cm/s
- Disassociation between mitral and tricuspid inflow patterns
- Significant change in mitral E/A ratio post-valsalva (> 50% change)
- Elevated PASP in absence of pulmonary disease (> 36 mmHg)
- Impaired global longitudinal strain (GLS) and reduced s’ velocity of LV
SUMMARY
Keep an eye out next week as we cover the next diastolic function algorithm for depressed ejection fraction!

Michael Owen RDCS, RVT
Connect with Michael: LinkedIn, iEchoToday
Check out iEchoToday’s Facebook
If you need additional information on how to obtain correct diastolic measurements check out CardioServ’s recent blog on Correct Techniques to Acquire Diastology Measurements. This article reviews how-to obtain:
- MV inflow
- Peak E-Wave Velocity (cm/s)
- Peak A-Wave Velocity (cm/s)
- A-Duration (msec)
- E/A Ratio
- Deceleration Time (msec)
- Pulmonary Veins
- S-Wave (cm/sec)
- D-Wave (cm/sec)
- AR Duration (msec)
- S/D Ratio
- LA Volume
- LV EF
- TR Velocity




