We dedicated the month of April to learning about ways to implement right heart quantification into our routine exams. This month, we are going to continue that journey and discuss ways to evaluate the function of the right heart!
“RV systolic function should be assessed by at least one or combination of the following: FAC, S’ Wave, TAPSE or RIMP.” –ASE JASE 2015
With that in mind, let’s jump into how to perform these!
The ASE explained 4 methods to quantify RV systolic function:
This week we are going to discuss how to perform TAPSE & S’ Wave measurements.
The reference values for these parameters do NOT provide a mild, moderate or severe value range. They do not take BSA, height or gender into consideration either. ASE provides us with normal and abnormal values.
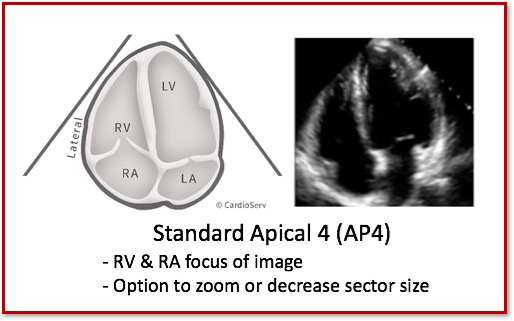
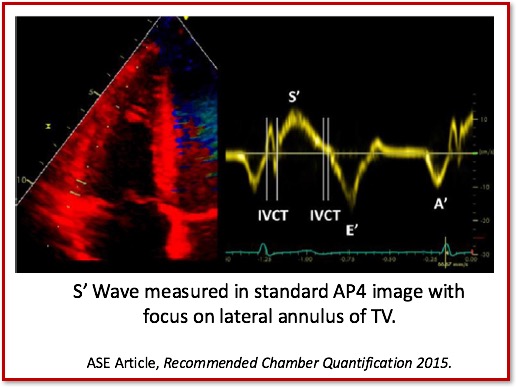
The ASE suggest using the standard AP4 window when performing RV function assessment.
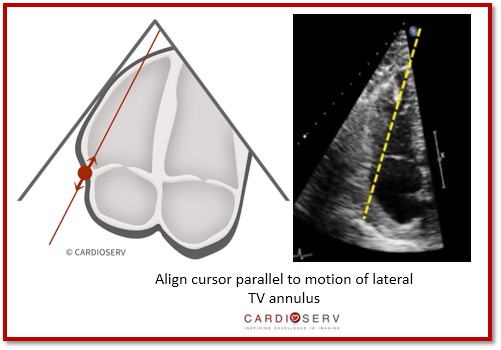
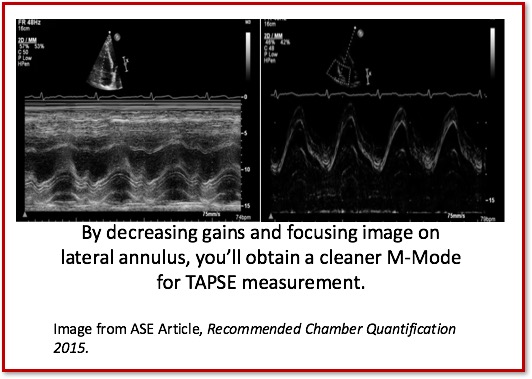
TAPSE is a linear M-Mode measurement of the RV longitudinal function.
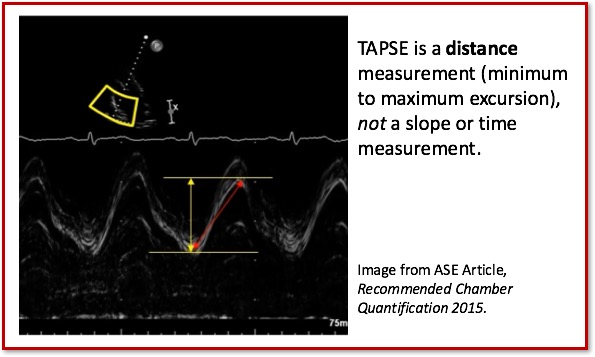
There were changes to the cutoff value for TAPSE in the latest ASE guidelines and ASE acknowledged that although there may be minor variations in TAPSE values according to gender and BSA that generally a TAPSE value less than 17mm is highly suggestive of RV dysfunction.
Peak systolic velocity of the tricuspid annulus by Pulsed Wave TDI (cm/sec).
Again, there were minor changes to the S’ reference range with the latest ASE guideline update. Just like TAPSE there are no values based upon mild, moderate or severe. The reference range provided is a cutoff range with a S’ value less than 9.5 cm/sec indicating RV dysfunction.
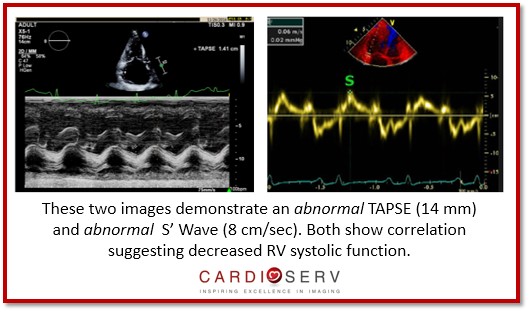
It is VITAL that we make sure we obtain both TAPSE and S’ Wave values to correlate together. If you are getting an abnormal TAPSE, then you need to make sure your S’ Wave is demonstrating an abnormal value as well.
Here is an easy reference chart to refer to in your scanning laboratory:
The ASE provides us with four great methods to use for evaluating the RV function. If you’re not using any method to quantify right heart function, today is the day to start! We at CardioServ, suggest using both TAPSE and S’ Wave. If you are only limited to one, S’ Wave is easily obtained and more reproducible. If you do get an abnormal S’ Wave, it would be idea to also perform a TAPSE as an additional method to proving your abnormal value. Next week, we will discuss two other methods [RIMP & FAC] we can use for evaluating right sided function!


Andrea Fields MHA, RDCS, Cardiac Clinical Director
Lang, R. M., MD, Badano, L. P., MD, & Mor-Avi, V., PhD. (2015). Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. JASE, 28(1), 1-53. Retrieved March 1, 2017, from http://asecho.org/wordpress/wp-content/uploads/2015/01/ChamberQuantification2015.pdf









May
2017
Oct
2020
May
2017
Apr
2019
May
2017
May
2017
May
2017
May
2017
Jun
2017
Jul
2017
Jul
2017
Aug
2017
Nov
2017
Nov
2017
Nov
2017
Nov
2017
Dec
2017
May
2018
Jun
2018
Sep
2018
Oct
2018
Oct
2018
Oct
2018
Oct
2018
Apr
2019
May
2019
Jun
2020
Jan
2021